

Approaches to Nonsurgical Root Canal Retreatment
These clinical strategies will help providers manage posttreatment endodontic disease
These clinical strategies will help providers manage posttreatment endodontic disease
Each year, millions of teeth with disease of the pulp and periradicular tissues are saved through endodontic treatment. Despite the high clinical success rates of nonsurgical root canal therapy, there are times when an endodontically treated tooth may exhibit posttreatment disease that requires further intervention. Posttreatment endodontic disease has four possible etiologies: microorganisms that are retained or reintroduced into the canal system, microorganisms that survive in the apical tissues outside the canal system, foreign body reactions in the apical tissues, and the presence of true periapical cysts.1,2 Treatment for intracanal microorganisms includes surgical and nonsurgical options, but the remaining three etiologies can only be treated surgically. Because it is often difficult to determine the causes of posttreatment endodontic disease, a thoughtful, evidence-based approach to treatment planning is necessary.
Treatment planning for diseased teeth is a complex process. A thorough dental history, clinical testing and radiographic examination are necessary to reach an accurate diagnosis. The introduction of three-dimensional imaging has had a significant impact on endodontic treatment planning. Limited field of view (FOV) cone beam computed tomography (CBCT) is the imaging modality of choice for teeth with posttreatment endodontic disease. The Joint Position Statement of the American Association of Endodontists and the American Academy of Oral and Maxillofacial Radiology3 states that limited FOV CBCT should be the imaging modality of choice when evaluating the nonhealing of previous endodontic treatment, as well as for nonsurgical retreatment to assess treatment complications or deficiencies that may have occurred during the previous endodontic therapy.
When compared to CBCT devices with larger FOVs, the smaller FOV generally provides higher resolution with less radiation exposure. And, unlike two-dimensional radiographs, due to its increased sensitivity in detecting roots with a periapical low density area, limited FOV CBCT enables clinicians to consider selective root retreatment, addressing only the roots with radiographic evidence of disease.4,5 Perhaps the most compelling evidence supporting the value of CBCT in endodontics comes from three studies showing that when CBCT data was added to otherwise complete diagnostic information, the subsequent treatment plan changed in 35% to 62% of cases.6–8
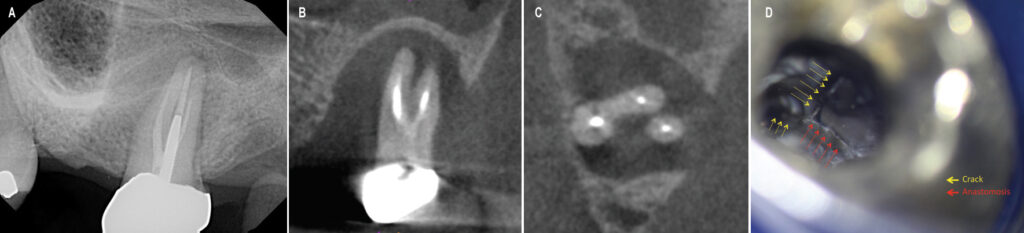
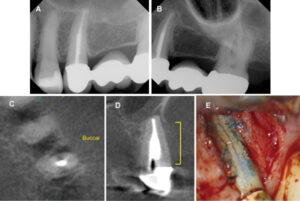
Limited FOV CBCT is useful in identifying untreated canals and root perforations, assessing complex anatomy (such as fins or fused roots), evaluating instrumentation and obturation quality, and visualizing bone loss patterns that are consistent with apical periodontitis, marginal periodontitis, furcation involvement or root fractures (Figures 1A through 1E).9 In many cases, situations can be discovered that would preclude successful endodontic retreatment, so that clinicians and patients can avoid the frustration of performing treatments that have a low chance of success (Figures 2A through 2D). After diagnosis, treatment options must be communicated to the patient so he or she can make an informed decision.
TREATMENT PLANNING DECISIONS
There are four options for managing a tooth with posttreatment disease: do nothing, extraction, nonsurgical retreatment, or surgical treatment.10 Avoiding treatment may result in the progression of disease and continued destruction of supporting tissues, as well as possible acute exacerbation of systemic side effects, such as cellulitis and/or lymphadenopathy. In most cases, these options are unacceptable. Extraction and replacement is a viable option, but replacements for missing teeth are rarely better than an otherwise restorable natural tooth,11 and nonreplacement usually results in unfavorable alternations in the adjacent dentition and surrounding tissues, as well as possible diminution of masticatory function. The decision of whether to perform nonsurgical or surgical retreatment to retain the tooth is also complex. The American Association of Endodontists offers a publication to help clinicians with these topics, Treatment Options for the Compromised Tooth: A Decision Guide (available at aae.org/treatmentoptions).
For most cases, the clinician needs to decide if retention of the tooth is in the patient’s best interest. This is based on the restorability of the tooth and its strategic position in the dentition, periodontal health, the patient’s health history, motivation and desires, and the skill level of the dentist.

Generally, the restorability of the tooth is determined by the amount of healthy and intact tooth structure that remains after careful removal of old restorations and caries or resorption. Important treatment planning questions when determining restorability include:
- Does adequate tooth structure remain to allow production of a ferrule for the restorative preparation?
- Will the margins of the potential restoration invade the biologic width?
- Will the remaining tooth structure be strong enough to resist fracture when occlusally loaded?
- Are there any preexisting tooth fractures or perforations of the root that may compromise the outcome?
- Will crown-lengthening surgery, if necessary (or even possible), expose a furcation or disturb the attachment height of adjacent teeth?
- Is it necessary to keep the tooth in order for the patient to masticate effectively, or will its loss result in the need for replacement?
- Does the site have adequate bone to retain a possible implant?
Patient factors are also critical in the decision to save or extract a tooth. Is the patient healthy enough to tolerate the treatment options? For example, patients with a history of medication use to treat osteoporosis and certain types of cancer may be at risk for medication-related osteonecrosis of the jaw, and the risk varies depending on the type of medication.12 In these patients, it is often advisable to avoid extraction surgery and retain the tooth via nonsurgical retreatment. Does the patient smoke or have diabetes? These conditions may affect outcomes of both root canal therapy and implant placement.13–17 Does the patient have the motivation and resources to retain a tooth or to place and restore an implant? Does the dental history reveal a problem with maintaining whichever treatment is selected? Can the patient tolerate the long appointment times needed to perform whichever treatment is selected? The clinician must answer these questions to help the patient make the best treatment decision for his or her particular situation.
RETREATMENT PROCEDURES
The procedures for endodontic nonsurgical retreatment can be grouped into disassembly, repair of existing perforations, access to missed anatomy, shaping and disinfection of the canal system, and obturation.10 While cleaning, shaping and disinfecting the root canal space in retreatment can be similar to initial root canal therapy, location and treatment of missed anatomy, disassembly, and perforation repair are complex procedures that require a specialized armamentarium and knowledge. The dental operating microscope allows clinicians to visualize the contents of canals and endodontic access preparations better than with loupes or the naked eye,18 and supports delicate retreatment procedures that cannot be accomplished by other means. Without the dental operating microscope and CBCT imaging, retreatment at the highest level is difficult — and sometimes impossible — to achieve.
When it comes to nonsurgical retreatment, intraoperative decision-making is typically complicated because what operators will find inside a treated tooth may be difficult to discern from the diagnostic data. “Expect the unexpected” is the general rule during retreatment, and clinicians must be prepared to adapt to each unique clinical situation.
An endodontically treated tooth often has a full coverage restoration. The clinician must decide whether to remove the coronal restoration or attempt to retain it by preparing an access through it. Removing an intact restoration with the aim of reusing it can be unpredictable. Most times, removal of the restoration is only considered when it needs to be replaced. The simplest approach is usually to prepare the access through the existing restoration — although this does pose the risk of damage that may require refabrication.19 It is prudent to warn the patient that retreatment may result in crown debonding or other damage that may require a new restoration.
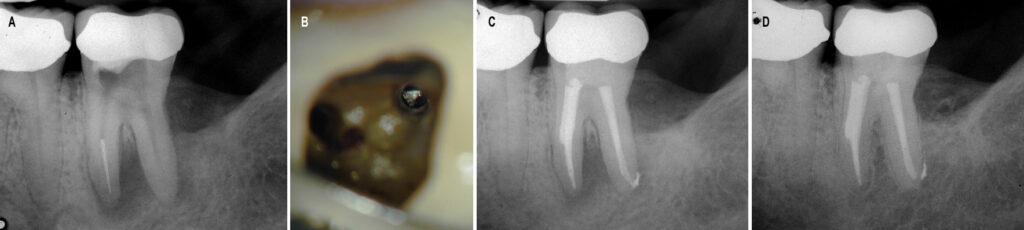
Generally, if a post and core are present, there is a high likelihood the coronal restoration will be lost. Endodontists use conservative access preparations to preserve as much tooth structure as possible, but a preexisting access in a tooth initially treated years ago will usually be larger. In addition, access enlargement often is necessary to excavate around and remove posts in the canals to be retreated. Post retrieval requires careful use of ultrasonic instruments to remove surrounding core material and disrupt the intracanal cement seal around the post.20 Care must be taken to avoid overheating the post because heat transmitted to the ligament during post removal may cause large areas of bone destruction and tooth loss.21–23 Intermittent application of the ultrasonic tip, along with copious air/water coolant spray, are necessary. There are numerous other instruments and techniques that can aid in the removal of a post, and the clinician should have training in, and access to, a wide selection to be able to retrieve posts in all situations (Figures 3A through 3E).
Following post retrieval, removal of preexisting root filling materials is necessary. The technique varies depending on the materials found in the canals.10 Removal of gutta-percha and solid-core obturators (with plastic or cross-linked gutta-percha carriers) usually is performed with some combination of heat, solvents, and endodontic files and reamers (both manual and engine-driven). Metal solid-core carriers usually require a different procedure because use of engine-driven instruments is contraindicated due to the risk of instrument breakage. Soft-paste root fillings require a crown-down technique to minimize extrusion of the potentially toxic paste components into the periradicular tissues, and hard pastes generally are removed with ultrasonics and solvents. Silver points are removed with endodontic files, forceps and special elevators, or a tube system.
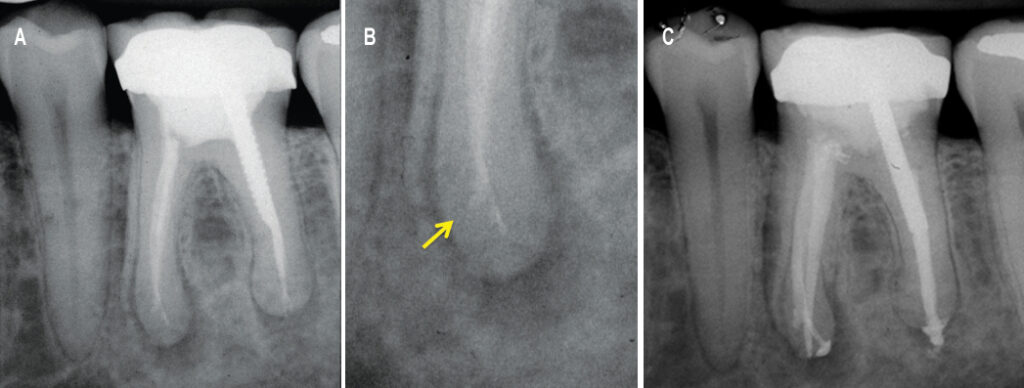
Occasionally, a separated instrument is found in the canal space. The presence of the separated instrument is not a direct cause of posttreatment disease; rather, the condition stems from necrotic pulp tissue or bacteria in the canal that cannot be removed because the separated instrument prevents disinfection.24 If a separated file in the canal is positioned coronally to the canal curvature, many times it can be removed successfully — but this requires a specialized armamentarium and techniques, including use of the dental operating microscope.25 Frequently, removal of tooth structure deep in the canal is required to access and remove the separated instrument. This can result in perforation of the root or weakening of the tooth structure, thus increasing chances of a future fracture (Figures 4A through 4D).
Root perforations (whether iatrogenic or resorptive) can cause periradicular periodontitis in root-treated teeth, and an assessment of whether the defect can be repaired is essential to effective treatment planning. Ideally, the perforation should be repaired as soon as possible,26 and repair of perforations below the periodontal attachment must be accomplished with bioceramic materials to enhance complete healing.27
After disassembly is complete, canals should be cleaned thoroughly and shaped for reception of new obturation materials. Due to iatrogenic canal irregularities (such as blockages, ledges, zips or canal transportation) from previous treatment, this is frequently a complicated process in teeth with posttreatment disease.28 Bypassing blockages and ledges, and thoroughly cleaning and disinfecting zipped or transported apical preparations, is difficult and time consuming (Figures 5A through 5C).10 Untreated canal ramifications (such as missed canals and lateral canals) are another challenge that needs to be addressed in retreatment, and each of these factors must be carefully managed to achieve a predictable outcome.29
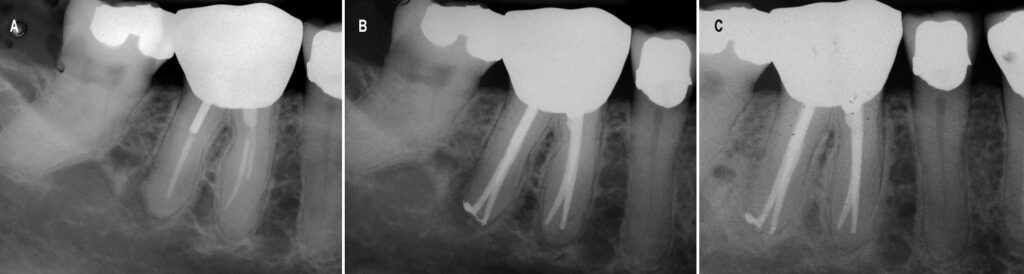
distal canal, and short fills of the mesial canals. Successful nonsurgical retreatment (B) resulted in complete healing and
an asymptomatic patient at the 19-month reevaluation (C).
The final step in retreatment is to thoroughly disinfect and three-dimensionally obturate the canal space. When these teeth are managed properly, complete healing rates for nonsurgical retreatment are high, ranging from 74% to 98%,30 while the patient’s quality of life and normal mastication are rapidly restored (Figures 6A through 6C).31
CONCLUSION
If retention of the tooth is the preferred treatment, general dentists may, in many cases, consider referral to an endodontist, as these practitioners have the training and equipment to plan and perform the highly specialized procedures needed to retain the tooth. What may not be obvious is that the endodontist is also the specialist who can be most helpful in deciding whether the tooth is restorable. The endodontist’s specialized training includes not only evidence-based treatment procedures, but also effective diagnosis and treatment planning for teeth with posttreatment endodontic disease. Highly experienced in “what works,” the endodontist will be the dentist’s most valuable partner in care when hard retreatment decisions are needed.
KEY TAKEAWAYS
- Limited field of view cone beam computed tomography (CBCT) is the imaging modality of choice for teeth with posttreatment endodontic disease.
- There are four options for managing a tooth with posttreatment endodontic disease: do nothing, extraction, nonsurgical retreatment, or surgical treatment.10
- The procedures for endodontic nonsurgical retreatment can be grouped into disassembly, repair of existing perforations, access to missed anatomy, shaping and disinfection of the canal system, and obturation.10
- Without the dental operating microscope and CBCT imaging, retreatment at the highest level is difficult — and sometimes impossible — to achieve.
- For most general practice situations, referral to an endodontist is advisable if retention of the tooth is the preferred treatment.
REFERENCES
- Sundqvist G, Figdor D. Endodontic treatment of apical periodontitis. In: Orstavik D, Pitt Ford T, editors. Essential Endodontology. Prevention and Treatment of Apical Periodontitis. London: Blackwell Science Ltd; 1998;242.
- Nair PN. On the causes of persistent apical periodontitis: a review. Int Endod J. 2006;39:249–281.
- Special Committee to Revise the Joint AAE/AAOMR Position Statement on use of CBCT in Endodontics. AAE and AAOMR joint position statement: use of cone beam computed tomography in endodontics 2015 update. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;120:508–512.
- Nudera WJ. Selective root retreatment: a novel approach. J Endod. 2015;41:1382–1388.
- Uraba S, Ebihara A, Komatsu K, Ohbayashi N, Okiji T. Ability of cone-beam computed tomography to detect periapical lesions that were not detected by periapical radiography: a retrospective assessment according to Tooth Group. J Endod. 2016;42:1186–1190.
- Ee J, Fayad MI, Johnson BR. Comparison of endodontic diagnosis and treatment planning decisions using cone-beam volumetric tomography versus periapical radiography. J Endod. 2014;40:910–916.
- Mota de Almeida FJ, Knutsson K, Flygare L. The effect of cone beam CT (CBCT) on therapeutic decision making in endodontics. Dentomaxillofac Radiol. 2014;43:20130137.
- Mota de Almeida FJ, Knutsson K, Flygare L. The impact of cone beam computed tomography on the choice of endodontic diagnosis. Int Endod J. 2015;48:564–572.
- Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic applications of cone-beam volumetric tomography. J Endod. 2007;33:1121–1132.
- Roda R, Gettleman B. Non-surgical retreatment. In: Hargreaves K, Berman L, eds. Cohen’s Pathways of the Pulp. 11th ed. St Louis: Elsevier;2015:324–386.
- Iqbal MK, Kim S. For teeth requiring endodontic treatment, what are the differences in outcomes of restored endodontically treated teeth compared to implant-supported restorations? Int J Oral Maxillofac Implants. 2007;22(Suppl):96–116.
- Ruggiero SL, Dodson TB, Fantasia J, et al. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw — 2014 update. J Oral Maxillofac Surg. 2014;72:1938–1956.
- Duncan HF, Pitt Ford TR. The potential association between smoking and endodontic disease. Int Endod J. 2006;39:843–854.
- Lopez-Lopez J, Jane-Salas E, Martin-Gonzalez J, et al. Tobacco smoking and radiographic periapical status: a retrospective case-control study. J Endod. 2012;38:584–588.
- Fouad AF, Burleson J. The effect of diabetes mellitus on endodontic treatment outcome: data from an electronic patient record. J Am Dent Assoc. 2003;134:43–51.
- Segura-Egea JJ, Martin-Gonzalez J, Cabanillas-Balsera D, Fouad AF, Velasco-Ortega E, Lopez-Lopez J. Association between diabetes and the prevalence of radiolucent periapical lesions in root-filled teeth: systematic review and meta-analysis. Clin Oral Investig. 2016;20:1133–1141.
- Chen H, Liu N, Xu X, Qu X, Lu E. Smoking, radiotherapy, diabetes and osteoporosis as risk factors for dental implant failure: a meta-analysis. PLoS One. 2013;8:e71955.
- Perrin P, Neuhaus KW, Lussi A. The impact of loupes and microscopes on vision in endodontics. Int Endod J. 2014;47:425–429.
- Mulvay PG, Abbott PV. The effect of endodontic access cavity preparation and subsequent restorative procedures on molar crown retention. Aust Dent J. 1996;41:134–139.
- Buoncristiani J, Seto BG, Caputo AA. Evaluation of ultrasonic and sonic instruments for intraradicular post removal. J Endod. 1994;20:486–489.
- Schwartz RS, Robbins JW. Post placement and restoration of endodontically treated teeth: a literature review. J Endod. 2004;30:289–301.
- Budd JC, Gekelman D, White JM. Temperature rise of the post and on the root surface during ultrasonic post removal. Int Endod J. 2005;38:705–711.
- Dominici JT, Clark S, Scheetz J, Eleazer PD. Analysis of heat generation using ultrasonic vibration for post removal. J Endod. 2005;31:301–303.
- Spili P, Parashos P, Messer HH. The impact of instrument fracture on outcome of endodontic treatment. J Endod. 2005;31:845–850.
- Gencoglu N, Helvacioglu D. Comparison of the different techniques to remove fractured endodontic instruments from root canal systems. Eur J Dent. 2009;3:90–95.
- Sinai IH. Endodontic perforations: their prognosis and treatment. J Am Dent Assoc. 1977;95:90–95.
- Main C, Mirzayan N, Shabahang S, Torabinejad M. Repair of root perforations using mineral trioxide aggregate: a long-term study. J Endod. 2004;30:80–83.
- Jafarzadeh H, Abbott PV. Ledge formation: review of a great challenge in endodontics. J Endod. 2007;33:1155–1162.
- Farzaneh M, Abitbol S, Friedman S. Treatment outcome in endodontics: the Toronto study. Phases I and II: orthograde retreatment. J Endod. 2004;30:627–633.
- Friedman S, Mor C. The success of endodontic therapy — healing and functionality. J Calif Dent Assoc. 2004;32:493–503.
- He J, White RK, White CA, Schweitzer JL, Woodmansey KF. Clinical and patient-centered outcomes of nonsurgical root canal retreatment in first molars using contemporary techniques. J Endod. 2017;43:231–237.
The author has no commercial conflicts of interest to disclose.
A version of this article originally appeared in ENDODONTICS: Colleagues for Excellence, Spring 2017. Reused with permission from the American Association of Endodontists, ©2017. The AAE clinical newsletter is available at aae.org/colleagues.
FEATURED IMAGE: MEDIAPHOTOS / ISTOCK / GETTY IMAGES PLUS
From Decisions in Dentistry. January 2018;4(1):21-24.

[…] https://decisionsindentistry.com/article/approaches-to-nonsurgical-root-canal-retreatment/ […]