Article Text

Abstract
Objectives We identified factors associated with thromboembolic and bleeding events in two contemporary cohorts of anticoagulated patients with atrial fibrillation (AF), treated with either vitamin K antagonists (VKA) or non-VKA oral anticoagulants (NOACs).
Design Prospective, multicentre observational study.
Setting 461 centres in seven European countries.
Participants 5310 patients receiving a VKA (PREvention oF thromboembolic events - European Registry in Atrial Fibrillation (PREFER in AF), derivation cohort) and 3156 patients receiving a NOAC (PREFER in AF Prolongation, validation cohort) for stroke prevention in AF.
Outcome measures Risk factors for thromboembolic events (ischaemic stroke, systemic embolism) and major bleeding (gastrointestinal bleeding, intracerebral haemorrhage and other life-threatening bleeding).
Results The mean age of patients enrolled in the PREFER in AF registry was 72±10 years, 40% were female and the mean CHA2DS2-VASc Score was 3.5±1.7. The incidence of thromboembolic and major bleeding events was 2.34% (95% CI 1.93% to 2.74%) and 2.84% (95% CI 2.41% to 3.33%) after 1-year of follow-up, respectively.
Abnormal liver function, prior stroke or transient ischaemic attack, labile international normalised ratio (INR), concomitant therapy with antiplatelet or non-steroidal anti-inflammatory drugs, heart failure and older age (≥75 years) were independently associated with both thromboembolic and major bleeding events.
With the exception of unstable INR values, these risk factors were validated in patients treated with NOACs (PREFER in AF Prolongation Study, 72±9 years, 40% female, CHA2DS2-VASc 3.3±1.6). For each single point decrease on a modifiable bleeding risk scale we observed a 30% lower risk for major bleeding events (OR 0.70, 95% CI 0.64 to 0.76, p<0.01) and a 28% lower rate of thromboembolic events (OR 0.72, 95% CI 0.66 to 0.82, p<0.01).
Conclusion Attending to modifiable risk factors is an important treatment target in anticoagulated AF patients to reduce thromboembolic and bleeding events. Initiation of anticoagulation in those at risk of stroke should not be prevented by elevated bleeding risk scores.
- atrial fibrillation
- anticoagulation
- thromboembolism
- major bleeding
- risk stratification
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We analysed a large and contemporary cohort of anticoagulated patients with atrial fibrillation (AF) enrolled across seven European countries.
Our findings were validated in a second, independent cohort of AF patients receiving a non-vitamin K antagonists oral anticoagulant for stroke prevention.
These datasets were analysed in a retrospective fashion; thus our findings have to regarded as hypothesis generating.
Introduction
Atrial fibrillation (AF) is a major risk factor for disabling stroke. Oral anticoagulation reduces the risk of stroke in patients with AF by almost two-thirds and is therefore recommended for most patients with AF.1 2
However, even on oral anticoagulation, stroke or systemic embolism occurs in 1%–4% of anticoagulated AF patients3–7 and approximately 2% experience a major bleed per year.8 Reducing this burden of residual adverse events is desirable to improve outcomes.
To date, conditions predisposing to thromboembolic3 9–18 and bleeding events4 18–22 in anticoagulated AF patients have not been fully investigated. Their identification could help to improve outcomes in anticoagulated patients with AF. We therefore sought to identify factors associated with thromboembolic events and major bleeding in AF patients treated with either vitamin K antagonists (VKA) or non-VKA oral anticoagulants (NOACs).
Methods
Study population
We analysed outcomes in anticoagulated patients enrolled into the PREvention oF thromboembolic events - European Registry in Atrial Fibrillation (PREFER in AF) registry.21 Baseline data were obtained from consecutive AF patients in seven European countries (Austria, France, Germany, Italy, Spain, Switzerland and the UK) between January 2012 and January 2013. Patients were included if they were at least 18 years of age and had a history of AF documented by electrocardiography or by an implanted cardiac device within the preceding 12 months.21
In order to reduce potential sources of bias and to achieve a cohort representative of the ‘real world’, no explicit exclusion criteria were defined. Investigators were encouraged to enrol patients consecutively to reduce selection bias.21 Patients receiving anticoagulation were included in the present analysis when information on outcome events was available during 1-year of follow-up.
We validated our findings in the independent PREFER in AF Prolongation cohort which contained 3156 AF patients treated with a NOAC, who were enrolled between June 2014 and May 2015.
This study was carried out in accordance with national law and the Declaration of Helsinki of 1975 (in its current revised form).
Outcome definitions
The combined ischaemic endpoint consisted of ischaemic stroke and systemic embolic events, including transient ischaemic attack (TIA), arterial embolism, venous thromboembolism or pulmonary thromboembolism.
The combined major bleeding endpoint included gastrointestinal bleeding requiring therapy, intracerebral haemorrhage and other life-threatening bleeding (resulting in substantial compromise requiring treatment). Outcomes were reported and adjudicated by the respective investigators at each site.
Statistical methods
Discrete characteristics are expressed as frequency counts and percentages. Continuous characteristics are expressed as means and SD or medians, where appropriate. Patients with missing data for outcome events or variables of interest were not included in the analysis.
Multivariable logistic regression with a stepwise inclusion of covariates was used to identify predictors for thromboembolic events and major bleeding, including components of the validated HAS-BLED and CHA2DS2-VASc risk stratification scheme and other variables available in the registry. For the best-performing clusters of thromboembolic events and major bleeding risk factors, optimal integer coefficients were estimated using combinatorial testing of all integer weights via a logistic regression stepwise selection model. Cross validation was performed using bootstrapping (1000× random splitting of the cohort in two parts of identical in size). Predictors and integer coefficients in the first cohort were validated in the second cohort (which was not used for coefficient fitting). The most frequent predictors and for those the most frequent integer coefficients were presented as optimal integer coefficients.
The average over 1000 runs is presented as bootstrapping area under the curve (AUC) together with variability estimation. Sensitivity analysis was performed by testing integer versus continuous coefficients, alternative age cut-offs, adequate rate control, rhythm control, presence of sinus rhythm, use of rhythm control therapy, presence of chronic kidney disease and different blood pressure cut-offs.
The receiver operating characteristic (ROC) contrast test was used to compare the predictive performance of the identified clusters of risk factors and established risk stratification schemes.23–26
The clusters of risk factors were independently validated in the PREFER in AF Prolongation Study, enrolling 3156 anticoagulated AF patients between June 2014 and May 2015. Patients enrolled into both studies (PREFER in AF and PREFER in AF Prolongation) were excluded from the validation cohort. Labile international normalised ratio (INR) was defined as unstable INR values <60% time in therapeutic range, as adjudicated and reported by the respective investigators at each site.
SAS V. 9.4 was used for all statistical analysis.
Patient involvement
Patients were not involved in planning, design and conduct of the PREFER in AF study. Results were disseminated through press releases by the funding body and the primary results of the PREFER in AF study are available through open access publication.21
Results
Patient characteristics
The PREFER in AF registry enrolled 7243 patients in 461 European centres.
The clinical characteristics of the anticoagulated primary analysis population with available 1-year follow-up (5310 patients) are reported in table 1. All patients received oral anticoagulation, of whom 7.4% were treated with a NOAC (dabigatran 64%, rivaroxaban 34%, apixaban 2%).
Clinical characteristics of the study population
At 1-year follow-up, there were 124 thromboembolic events, with a corresponding annual rate of 2.34% (95% CI 1.93% to 2.74%) (table 2).
Incidence of thromboembolic events in the PREvention oF thromboembolic events - European Registry in Atrial Fibrillation (PREFER in AF) study (derivation cohort) and the PREFER in AF Prolongation Study (validation cohort)
In total, 151 (2.84%, 95% CI 2.41% to 3.33%) major bleeding events occurred in 145 patients. Of these, 74 (1.39%, 95% CI 1.10% to 1.75%) were gastrointestinal bleeding, 15 (0.28%, 95% CI 0.16% to 0.47%) were intracerebral haemorrhages and 68 (1.28%, 95% CI 1.00% to 1.62%) were other life-threatening or major bleeding requiring therapy (six patients experienced more than one bleeding episode).
Best-performing cluster of risk factors for thromboembolic events
On multivariable analysis a best-performing cluster of risk factors for thromboembolic events was identified. In descending order of relative risk, the inputs were abnormal liver function, prior stroke or TIA, labile INR, concomitant therapy with antiplatelet or non-steroidal anti-inflammatory drugs (NSAIDs), heart failure and age ≥75 years (table 3, figure 1).
Risk factors for thromboembolic events in anticoagulated atrial fibrillation patients, presented as ORs with 95% CIs (PREvention oF thromboembolic events - European Registry in Atrial Fibrillation derivation cohort). *Concomitant therapy with antiplatelet agents or non-steroidal anti-inflammatory drugs. INR, international normalised ratio; TIA, transient ischaemic attack.
Risk factors associated with thromboembolic events (PREvention oF thromboembolic events - European Registry in Atrial Fibrillation derivation cohort)
Ninety-five per cent of patients with a labile INR received a VKA during the entire follow-up period, thus, the confounding effect of patients switched to a NOAC was insignificant.
Adequacy of rate control, the presence of sinus rhythm on follow-up, use of antiarrhythmic drugs, chronic kidney disease and alternative age cut-offs did not improve the score. Uncontrolled hypertension levels were low (only 3.3% of patients >160 mm Hg at 1 year), diminishing a statistical impact on multivariable modelling.
The C-index with respect to the combined endpoint of thromboembolic events was 0.7402 (95% CI 0.6868 to 0.7935, p<0.01 vs HAS-BLED) (online supplementary table 1).
Supplementary
Sensitivity analysis for a combined ischaemic endpoint excluding TIA, as well as for TIA only, show numerically consistent results (online supplementary tables 2 and 3).
Best-performing cluster of major bleeding risk factors
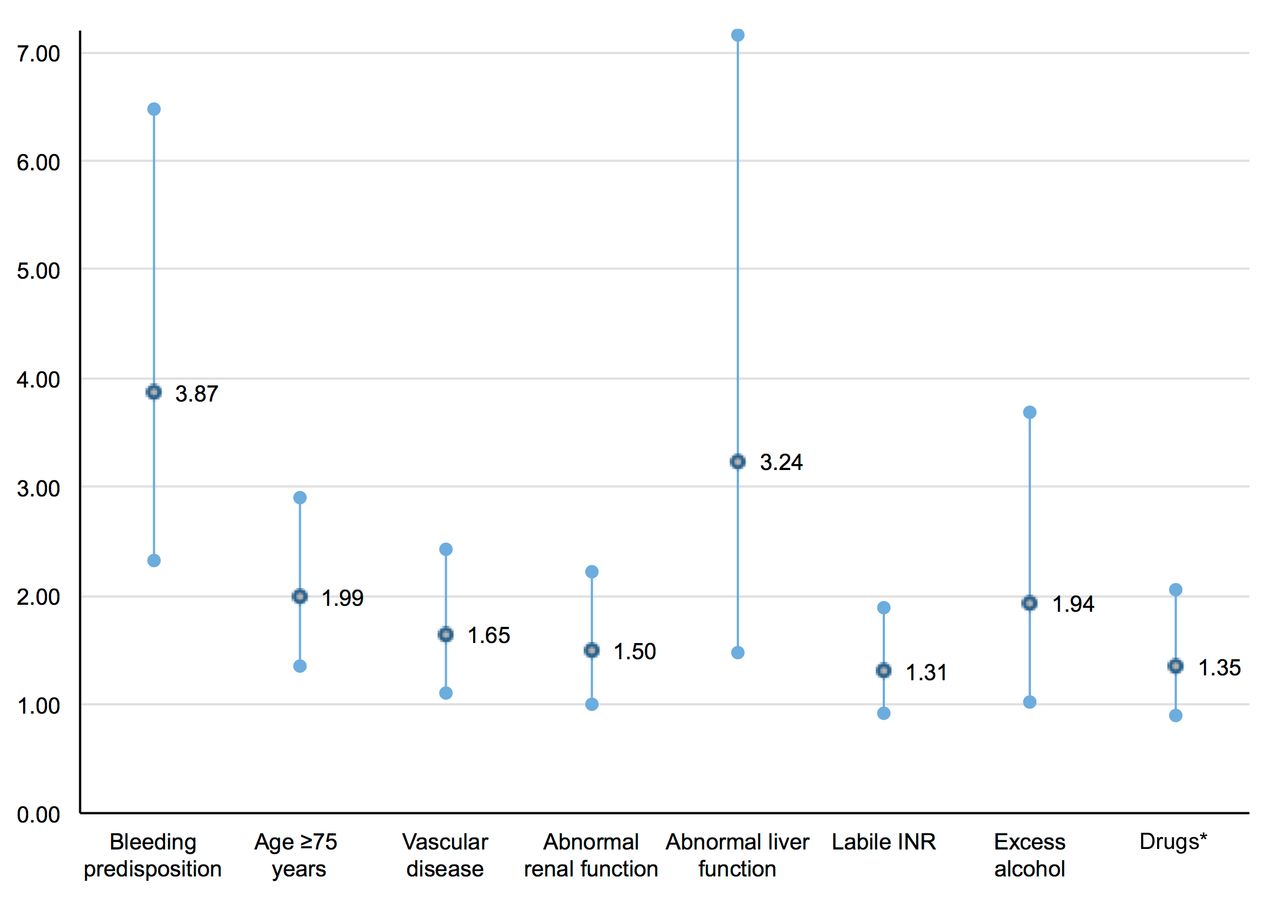
The best-performing cluster of major bleeding risk factors included modifiable inputs of the HAS-BLED score (except for hypertension, due to low exposure to elevated blood pressure levels), a modified age cut-off and vascular disease (table 4, figure 2). The C-index for major bleeding was 0.6982 (95% CI 0.6529 to 0.7469, p<0.01 vs HAS-BLED) (online supplementary table 1).

{kind=link}
{kind=link}
Risk factors for major bleeding events in anticoagulated atrial fibrillation patients, presented as ORs with 95% CIs (PREvention oF thromboembolic events - European Registry in Atrial Fibrillation derivation cohort). *Concomitant therapy with antiplatelet agents or non-steroidal anti-inflammatory drugs. INR, international normalised ratio.
Risk factors associated with major bleeding (PREvention oF thromboembolic events - European Registry in Atrial Fibrillation derivation cohort)
For each single point decrease in this cluster of mostly modifiable bleeding risk factors we observed a 30% lower relative risk for major bleeding events (OR 0.70, 95% CI 0.64 to 0.76, p<0.01). When applied to evaluate the risk for thromboembolic events, there was a 28% lower event rate per point decrease on this adjusted modifiable bleeding risk scale (OR 0.72, 95% CI 0.66 to 0.82, p<0.01).
Based on this observation, for each single point decrease on this best-performing scale of modifiable bleeding risk factors, we estimate a number needed to treat (NNT) of 111 to prevent one major bleeding event (0.9% absolute risk reduction) and an NNT of 143 to prevent one ischaemic event (0.7% absolute risk reduction) during 1-year of treatment.
Validation in the PREFER Prolongation Study
The identified clusters for thromboembolic and major bleeding events were independently validated in the PREFER Prolongation Study, which enrolled 3156 AF patients receiving a NOAC for stroke prevention. Rivaroxaban was used in 50%, apixaban in 26% and dabigatran in 24% of patients. Clinical characteristics were similar to the derivation cohort in terms of age (72±9 years), gender (40% female), stroke risk (CHA2DS2-VASc 3.3±1.6) and bleeding risk (HAS-BLED 1.9±1.1) (table 1).
Labile INR was reported in 6.9% of patients in the validation cohort and validation was performed disregarding labile INR, as well as accounting for labile INR as a surrogate for poor compliance.
The clusters of risk factors for thromboembolic events and major bleeding had numerically higher c-indices than established risk scores for the respective outcomes, consistent with results from the derivation cohort (online supplementary table 4). Lower absolute c-indices and non-significant differences regarding the predictive performance between the scores are reflected by a lower sample size and a lower incidence of outcome events in the validation cohort.
Validation results were consistent when labile INR was accounted for as a surrogate for poor compliance (online supplementary table 5).
Discussion
The main finding of this study is that in a large cohort of anticoagulated AF patients, modifiable risk factors can be attributed to a substantial proportion of both thromboembolic and major bleeding events. In addition, this analysis confirmed other risk factors for embolic and bleeding events in anticoagulated AF patients such as prior stroke, older age and heart failure. Major modifiable factors were labile INR values (in patients treated with VKA), concomitant therapy with antiplatelet agents or NSAIDs and as a potentially modifiable risk factor liver damage.
The modifiable risk factors identified here overlap with modifiable bleeding risk factors highlighted in the 2016 European Society of Cardiology (ESC) AF guidelines (uncontrolled hypertension, labile INR, antiplatelet drugs or NSAIDs and excess alcohol intake).1 Our estimates suggest that patients in whom modifiable bleeding risk factors are minimised as part of an integrated management approach for AF might also be at lower risk for thromboembolic events.9–17 Also in line with previous data, our analysis demonstrates that the CHA2DS2-VASc score was inferior in terms of bleeding risk prediction compared with the HAS-BLED score and should not be used to estimate bleeding risk in anticoagulated AF patients.19 20 27
Simple measures that could be helpful to reduce residual thromboembolic and major bleeding events in anticoagulated patients suggested by our analysis include:
Switching from a VKA to a NOAC in patients with labile INR values.
Timely discontinuation of antiplatelet therapy and minimisation of treatment with NSAIDs.
As shown previously, patients with well controlled INR values have a significantly lower risk for adverse cardiovascular outcomes. Adding time in therapeutic range to established bleeding risk stratification schemes such as the ATRIA and ORBIT score significantly improved their predictive performance.28–30 This further underlines the importance of a high-quality anticoagulation control in case VKA are used and the need for adequate adherence to NOACs.31
Blood pressure was well controlled in our cohorts, thus limiting our ability to quantify the impact of uncontrolled hypertension on thromboembolic events and major bleeding.1 32
Successful treatment of chronic kidney or liver disease may contribute to improve outcomes.1 33 Liver disease may also be a proxy for alcohol abuse, a factor that has been associated with bleeding in other cohorts.34
Our results also support the concept that the initiation or withdrawal of anticoagulation should not be based on bleeding risk, as stroke risk and bleeding risk are intricately linked. Instead, the increasing returns in terms of net clinical benefit—by treating subjects with greater thromboembolic risk—should be considered when initiating oral anticoagulation in AF patients.4 35 36 Importantly, we have been able to validate our findings in a cohort of AF patients anticoagulated with NOACs.
Limitations and strengths
The management of patients in included in the PREFER in AF registry is well aligned with evidence-based therapy and current treatment guidelines, underlining the generalisability of our findings in contemporary clinical practice. Worth mentioning, the derivation and validation cohort were recruited consecutively, thus in different periods in time (January 2012–January 2013 and June 2014–May 2015). We cannot fully explain the association of the risk factors identified in this analysis with both major bleeding and thromboembolism. Importantly, our findings are based on associations and hence hypothesis-generating. While we were able to validate our findings in an independent cohort, interventional trials testing the simple interventions identified in our analysis are desirable to assess their effect on thromboembolic and major bleeding outcomes.
While it seems intuitive that labile INR values predispose to both bleeding and stroke, it is less clear how concomitant therapy with antiplatelet agents or NSAIDs can contribute to stroke risk. It is conceivable that bleeding events led to temporary disruption of anticoagulation, thereby increasing the risk for thromboembolic events. In addition, concomitant therapy with these substances could be a marker for patients at higher risk of ischaemic events due to confounders that were not captured in our data set.
Conclusion
A substantial number of thromboembolic and major bleeding events in anticoagulated patients with AF can be attributed to a few modifiable risk factors. For each single point decrease on an adjusted modifiable bleeding risk scale, we observed an approximately 30% reduction in both major bleeding and thromboembolic events.
Our findings suggest that normalising INR, avoiding exposure to antiplatelet agents or NSAIDs and preventing liver disease could reduce both bleeding and residual stroke risk in AF patients receiving anticoagulation.
Acknowledgments
This analysis of the PREFER in AF registry was initiated by the Thrombosis Exchange Meeting in AF, TEAM in AF, funded and sponsored by Daiichi-Sankyo Europe. We would like to thank all centres that participated in this registry and all patients who gave their consent to participate.
References
Footnotes
Contributors MR contributed to the statistical analysis and prepared the manuscript draft. TWW contributed to the statistical analysis and reviewed the manuscript draft. LP performed the statistical analysis. GP contributed to the design of the present analysis and reviewed the manuscript draft. JMSM contributed to the design of the present analysis and reviewed the manuscript draft. RBS contributed to the design of the present analysis and reviewed the manuscript draft. RS was involved in the conduct of the PREFER in AF study, contributed to the design of the present analysis and reviewed the manuscript draft. DK contributed to the design of the present analysis including statistical consideration and reviewed the manuscript draft. ML was involved in the funding and conduct of the PREFER in AF study and the present analysis. KH contributed to the design of the present analysis and reviewed the manuscript draft. RDC was involved in the conduct of the PREFER in AF study, contributed to the design of the present analysis and reviewed the manuscript draft. PK was involved in the conduct of the PREFER in AF study, contributed to the design of the present analysis including statistical consideration and reviewed the final manuscript draft.
Funding The PREFER in AF study was supported by Daiichi-Sankyo Europe.
Competing interests MR received advisory fees from Daiichi Sankyo and Novarits and lecutring fees from Biotronik and Takeda Pharma. TWW received lecturing fees and advisory honoraria from Daiichi Sankyo, Boehringer Ingelheim and Pfizer/BMS. LP consultant fees from Daiichi-Sankyo, SOTIO, Beckman Coulter, Novartis. GP speaker/consultant/advisory board for Amgen, Sanofi, Bayer, Boehringer-Ingelheim, BMS-Pfizer, Daiichi Sankyo, Astra Zeneca, Sigma-Tau, Malesci, PIAM and MSD. JMSM lecture or consultant fees from AstraZeneca, Daiichi Sankyo, Eli Lilly, Bayer and research grant from Roche Diagnostics. Menarini and lecture fees from AtriCure, all outside the submitted workML is affiliated with the sponsor. KH received lecturing fees and advisory honoraria from Boehringer Ingelheim, Pfizer/BMS, Bayer, Daiichi Sankyo, Sanofi-Aventis, AstraZeneca, and Eli Lilly. RDC received research grants from Boehringer-Ingelheim, Bayer and BMS/Pfizer. Honoraria for lecturing and participation to Advisory Boards from Boehringer-Ingelheim, Bayer and BMS/Pfizer, Daiichi-Sankyo, Lilly, AstraZeneca, Merck, Novartis, Roche. PK has received research support from European Union, British Heart Foundation, Leducq Foundation, Medical Research Council (UK), and German Centre for Heart Research, from several drug and device companies active in atrial fibrillation, and has received honoraria from several such companies. PK is listed as inventor on two patents held by University of Birmingham (Atrial Fibrillation Therapy WO 2015140571, Markers for Atrial Fibrillation WO 2016012783).
Ethics approval Ethics committees in the respective seven participating European countries, as listed in the online supplementary appendix.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Main results from the PREFER in AF study are accessible from DOI 10.1093/europace/eut263.
Patient consent for publication Not required.