

March 2023 Volume 15 Issue 3 THE INDEPENDENT VOICE OF PHARMACY TEAM TRAINING: Dehydration Page 76 PHARMACYNEWSIRELAND.COM ROBBIE HENSHAW
LIVE THE WAY is available exclusively from www.uniphar.ie (01) 468 7501 A DIVISION OF linkup@uniphar.ie This Publication is for Healthcare Professionals Only
Irish International Rugby Player


* 150mg CoQ10 3,000mg L-Arginine IMMUNE SYSTEM ENERGY HEART IMMUNE SYSTEM ENERGY HEARTIMMUNE SYSTEM ENERGY HEART THE POWER OF ONE SACHET Call: 091 769803 | Email: customerservice@reviveactive.com | Web: reviveactive.com
Page 4: Boots
Pharmacy Ireland opens two new stores



Page 6: Medicine shortages continue to persist
Page 10: Calls for Strategy to improve patient care
Page 14: Superintendent
Pharmacist Ronan Ward on his career progression
Page 16: A Guide to Baby Skin Care
Page 24: Fertility training for pharmacists
Page 38: IPHA welcomes publication of the Mazers Report
Page 46: Launch of the Irish Pharmacy Awards 2023 Categories
PUBLISHER:
IPN Communications
Ireland Ltd.
Clifton House, Fitzwilliam Street
Lower, Dublin 2 00353 (01) 6690562
MANAGING DIRECTOR
Natalie Maginnis n-maginnis@btconnect.com
EDITOR
Kelly Jo Eastwood: 00353 (87)737 6308 kelly-jo@ipn.ie
ADVERTISING EXECUTIVE
Amy Evans: amy@ipn.ie
EDITORIAL/ EVENTS & MARKETING EXECUTIVE
Aoife Hunter: aoife@ipn.ie
CONTRIBUTORS
Theresa Lowry-Lehnen
Helena Tubridy
Katie Mugan
Dr Madelaine Jackson
Dr Annemarie Bennett

Christine Newman
Professor Fidelma Dunne
Motty Varghese
Dr Laura Lenihan
Dr Kate Gilmore
Dr Sarah Fitzgibbon
Jemma Henry
DESIGN DIRECTOR
Ian Stoddart Design
Foreword
In one of our lead news stories this issue, the pharmacy profession has welcomed plans to increase the number of education places for pharmacists in Ireland. Ireland has not been training enough pharmacists in recent years, which according to the IPU is resulting in growing pressures on the sector.
Media reports have suggested that Minister for Health, Stephen Donnelly, has called on the Higher Education Authority (HEA) to increase the number of training places. The HEA is said to have issued an expression of interest to education institutes to provide additional training. Welcoming the development, IPU Secretary-General Sharon Foley said, “Ireland currently has not got enough qualified pharmacists to support an ageing population and growing demands on the community pharmacy sector with graduating pharmacists in Ireland per 100k population below the OECD average (3.45 Vs 4.23). Traditionally, Ireland has relied on the UK and other countries to train our healthcare workers, in particular pharmacists. But we must, as a country, take ownership over educating key workers such as pharmacists.”
A Pathway to Success!
Turn to page 5 for the full story.
Elsewhere, and on page 6 we detail how medication shortages are continuing to cause issues. According to the latest Medicine Shortage Index, 247 different medicines used by Irish patients are currently out-of-stock, as a new trend affecting supply develops.
The latest figures show the number of medicine shortages in Ireland up an additional 19 medicines in short supply since the end of last month, and a 38% increase since the Index began in October. Of the 247 medicines currently unavailable, 13 are listed on the World Medical Organisation’s (WHO) ‘critical medicines’ list.
Meanwhile, the decision by Minister for Health, Stephen Donnelly T.D. to publish the Mazars Report has been welcomed by the Irish Pharmaceutical Healthcare Association as a positive step towards providing Irish patients with faster access to lifechanging new medicines. You can read more about this on page 38.
On a more positive front, this issue sees the launch of the 2023 Irish Pharmacy Awards, which details on all of the categories ranging from the Reckitt Community Pharmacist of the Year to the Théa Pharma OTC Counter Assistant of the Year Award. Full details on each are on pages 46 onwards, with further information on eligibility and how to enter.
I hope you enjoy the issue.
Regulars
circulated to all independent, multiple Pharmacists and academics in Ireland.
All rights reserved by Irish Pharmacy News. All material published in Irish Pharmacy News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission. IPN Communications Ltd. has taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
CPD: SLEEP DISORDERS
FEATURE: CERVICAL CANCER
FEATURE: OBESITY MANAGEMENT
TEAM TRAINING: DEHYDRATION
P41
P65
P74


P76
CLINICAL PR: P80
3 PHARMACYNEWSIRELAND.COM
SuperIntendent Pharmacist Ronan Ward talks to us about his career progression
is
Irish Pharmacy News
IRISH PHARMACY NEWS 4 14
PHARMACYNEWSIRELAND.COM @Irish_PharmNews IrishPharmacyNews Contents 46
New Pharmacy Appointments
The Pharmaceutical Society of Ireland (PSI), the pharmacy regulator confirms that the nomination process for pharmacists for appointment to the PSI Council is now open. PSI-registered pharmacists interested in making a public service contribution by participating in the work of the regulator at board-level, should consider the information available now on the PSI website. The nomination period is open until March 22nd.
The PSI Council is the governing body of the pharmacy regulator, comprising of 21 members. The PSI Council is responsible for the delivery and implementation of the regulator’s Corporate Strategy and for ensuring that the pharmacy regulator fulfils its statutory remit in the public interest.
There will be several vacancies on the Council this June and four of these for pharmacist members, who are appointed through the nomination and election process. The current pharmacist Council members concluding their respective terms of office are Mr. Roy Hogan, Mr. Mark Jordan, PSI President Ms. Muireann Ní Shúilleabháin and Ms. Avril Ryan.
Interested candidates, who must be on the PSI Register of Pharmacists, are invited to
submit a nomination form to the PSI Returning Officer by 12noon on Wednesday, March 22nd. In the event of the nominations exceeding the number of vacancies available, an election will be held on April 19th.
Each member of the PSI Council is appointed by the Minister for Health to act in the interest of patients and the public to assure safe and effective pharmacy practice and care in Ireland.
Further information on submitting a nomination and the relevant criteria is available on www.psi.ie
Katherine Morrow joins APPEL
Katherine Morrow has recently joined the board of APPEL (Affiliation for Pharmacy Practice Experiential Learning). She joins in
Boots Ireland Open New Stores
the position of new Director and National Coordinator.
Katherine brings a wealth of experience to the role, having most recently worked as Operations Director for the Irish Institute of Pharmacy and subsequently as Head of Education & Professional Competence at the Irish College of General Practitioners. Katherine has significant experience in all areas of practice including community, hospital, and regulatory, and is passionate about driving quality standards in education and development.
Following Joanne Kissane’s much-valued tenure with APPEL, Katherine is committed to continuing to support and evolve the APPEL programme and looks forward to connecting with you over the coming months.
Boots Ireland has announced the opening of two new stores in Harold’s Cross and Deansgrange in Dublin. As part of Boots continued investment into the growth and expansion of stores around the country, the two store openings brings the total number of Boots stores in the Republic of Ireland to 93.
Stephen Watkins, Managing Director of Boots Ireland with Joe Scallan, Head of Stores Boots Ireland and colleagues from the newly opened Boots Store in Harold’s Cross, Sarah Gaffney, Yasmin Kirby and Meadhbh Honohan

HRB Impact Award
The Health Research Board has presented their Impact Award 2023 to Orla Hardiman, Professor of Neurology at Trinity College, Consultant Neurologist at Beaumont Hospital, and National Clinical Lead, Neurology, at the Health Services Executive.
The prestigious award –selected by an international panel - recognises how Orla’s exceptional contribution to research has informed policy and practice in a way that positively impacts both the care and the well-being of patients living with neurodegenerative conditions and their families.
Professor Hardiman said, “I am grateful and humbled to be nominated for the HRB Impact Award by Professor Doherty at Trinity College Dublin and Ms Magdalen Rogers of the Neurological Alliance of Ireland. My genuine hope is that I, and our research group, have made an impact that will outlast our own professional careers and that we will in the future be able to say that ALS/MND is a chronic, rather than a fatal, condition.”
Explaining the driving force behind her research, Orla said, “Very early in my professional life, I made a conscious decision that all of my research endeavours would be guided by my experience as a working clinician, and by my desire to improve the lives of those whom I have the privilege of serving as a Consultant Neurologist.
The Harold’s Cross store, located at 280 Harold’s Cross Road in Dublin 6 opened its doors this week and will employ 14 people. Customers will have access to pharmacy services including prescription services, blood pressure testing and emergency contraception with additional services planned over the coming months.
Based on Clonkeen Road, Deansgrange, the former Grange Pharmacy was acquired by Boots last year and has since undergone refurbishment works to offer customers an extended offering of beauty, health, and wellness products, as well as a broader range of pharmacy services. The new store in Deansgrange
employs 13 people in the locality, including members of the original Grange Pharmacy team.
Commenting on the opening of the new stores, Stephen Watkins, Managing Director of Boots Ireland said, “Boots Ireland is continuing to expand its comprehensive offering to customers and patients in the local communities across Ireland, with the latest store openings in Deansgrange and Harold’s Cross brining our total number of stores in the country to 93. This is an exciting milestone to begin the year with, and I wish the teams in both stores every success.”
“My guiding light throughout my research career has been to continuously ask myself whether the research work we do “matters” in a real-world sense to those we serve?
“In my clinical career I have tried to improve both the lot of people with chronic neurologic disease and to enhance clinical services for those with ALS/ MND and related disorders.”
From her early days to her current role as National Clinical Lead in Neurology for the Health Service Executive, Professor Hardiman has been an inspirational leader who has ensured that research delivers for health.
PHARMACYNEWSIRELAND.COM 4 News
CAYA Annual Report
The HSE the National Cancer Control Programme (NCCP) has launched the second children, adolescent and young adult (CAYA) cancer program Annual Report 2022. The report highlights progress and achievements in the area of adolescent and young adult (AYA) cancer care during 2022.
A key focus in 2022 was publishing and implementing the recommendations set out in the Framework for the Care and Support of Adolescent and Young Adults (AYA) with Cancer in Ireland.
Key Messages for 2022
‘The Hangout’ A six month pilot programme aimed to create a non-clinical environment for Adolescent and Young Adult cancer patients commenced in 2022.
• Establishment of Young Persons Advisory Group (YPAG) at National Children’s Cancer Service. This service will ensure that children and young people with cancer will have a voice, share their opinions, and be actively involved in the design and delivery of clinical research and services, to make sure they are relevant and suited to their needs.
• Enabling access to CAYA Cancer Patients blood results via Healthlink between Children’s Health Ireland (CHI) at Crumlin, Mercy University Hospital and Our Lady of Lourdes Hospital, Drogheda.
• A Model of Care for PsychoOncology Services for CAYA with cancer and their families began development in 2022.
• The NCCP welcomed the inclusion of childhood, adolescent and young adult cancer in the ‘significant ongoing illness’ criteria of DARE (Disability Access Route to Education). DARE is an alternative admissions route to third level for students whose disability or ongoing illness has had a negative impact on their second level education.
• Delivery of education on AYA palliative care for Royal College of Physicians Ireland and to both pediatric and adult based healthcare services.
Keane’s CarePlus - Best Place to Work Accolade
Keane’s CarePlus Pharmacy Group is thrilled to announce that it has been recognised as the Best Place to Work in Ireland. In addition, the company has also received two notable accolades - the highest-ranked pharmacy group overall and the 16th best place to work in the small business category.
The recognition as the Best Place to Work in Ireland is a testament to the company’s unwavering dedication to creating a supportive and positive workplace culture for its employees. John Keane, CEO and Owner of Keane’s CarePlus Pharmacy Group, expressed his gratitude for the award, stating, “We are extremely proud and honoured to receive this recognition. It demonstrates that our team’s hard work and dedication have paid off, and we will continue to invest in our people and culture.”
Furthermore, the recognition as the highest-ranked pharmacy group overall and the 16th best place to work in the small business category reflects the company’s continued commitment to creating a positive and supportive environment for its employees.
Gillian Ryan, COO of Keane’s CarePlus Pharmacy Group, expressed her delight in achieving these awards, saying, “We are thrilled to be recognised as one of the best places to work in the

small business category and the highest-ranked pharmacy group overall. We believe that investing in our people and culture allows us to provide the best service to our patients and customers.”
Keane’s CarePlus Pharmacy Group is committed to providing a positive work environment and exceptional customer service to its patients and customers.
Welcome for Increase in Pharmacy Places
The Irish Pharmacy Union (IPU) has welcomed plans to increase the number of education places for pharmacists in Ireland. Ireland has not been training enough pharmacists in recent years, which according to the IPU is resulting in growing pressures on the sector.
Media reports have suggested that Minister for Health, Stephen Donnelly, has called on the Higher Education Authority (HEA) to increase the number of training places. The HEA is said to have issued an expression of interest to education institutes to provide additional training.
Welcoming the development, IPU Secretary-General Sharon Foley said, “Ireland currently has not got enough qualified pharmacists to support an ageing population and growing demands on the community pharmacy sector with graduating pharmacists in Ireland
per 100k population below the OECD average (3.45 Vs 4.23). Traditionally, Ireland has relied on the UK and other countries to train our healthcare workers, in particular pharmacists. But we must, as a country, take ownership over educating key workers such as pharmacists.
“While we welcome the Minister’s ambition to increase the availability of training places this year it is imperative that there is a prompt response confirming the number of new places available and also any initiatives being undertaken to improve workforce
planning. We would encourage all suitably experienced HEIs to engage in this process and the Irish Pharmacy Union is available to offer any practical support that may be of benefit.”
“This coming September will see at least a further additional 60 medicine places again and quite possibly more,” a spokeswoman for Mr Harris told The Irish Times. “In addition, medical education will be provided on an all-island basis and Minister Harris hopes to be able to announce the details very shortly.”
PHARMACYNEWSIRELAND.COM 5
News
Robert Keane and the team from Keane’s CarePlus Pharmacy Group
Medicine shortages continue to Persist
Medicine shortages in Ireland continue to persist with 247 different medicines used by Irish patients currently out-of-stock, as a new trend affecting supply develops, according to the latest Medicine Shortage Index.
The latest figures show the number of medicine shortages in Ireland up an additional 19 medicines in short supply since the end of last month, and a 38% increase since the Index began in October.
Of the 247 medicines currently unavailable, 13 are listed on the World Medical Organisation’s (WHO) ‘critical medicines’ list.
The latest shortages analysis indicates a new trend of medicines that are stored or delivered using plastic components now increasingly in short supply. These medicines include nasal sprays, inhalers for the treatment of asthma and 11 different eye drop products.
Other medicines still in short supply across multiple suppliers in the past week include those that treat epilepsy, and medicines used for the treatment of high blood pressure.
Many antibiotics like Amoxicillin and Penicillin and commonly used over-the-counter medicines like Benylin ™ and Dioralyte ™ are still difficult for patients to source.
The Medicine Shortage Index, prepared by industry experts, Azure Pharmaceuticals, analyses data made publicly available by the Health Products Regulatory Authority (HPRA).
Other European countries have already taken specific policy measures to date in response to the escalating medicine shortage issue. Portugal, the UK, Germany, and Switzerland have all taken a range of price related policy measures in response to the problem, including price increases for lower priced medicines.
While, Sweden, Denmark and Malta, which all use tenders to set reimbursement prices, have all experienced price increases due to lack of supply of core medicines. To date, the Irish
Department of Health is yet to meaningfully respond to this deepening challenge.
Medicine shortages will continue grow incrementally unless political will is shown in Ireland to take measures, like those carried out by other EU nations, to meaningfully tackle the issue, Sandra Gannon, Azure CEO, said: “One of the means we have to protect our domestic supply of stock, to prevent these important medicines from running out, is through pricing. Other European countries have already recognised this fact and taken measures to mitigate against situations where their stocks run out. For example, Portugal recently raised its pricing by up to 5% for cheap medicines.
“Weaknesses in the supply chain alone highlight the imperative of revisiting the pricing framework for medicines to protect supply of stock and protect Irish patients.”
Award Shortlisting for PHONEIX Group
The Irish Businesses, owned by the PHOENIX Group, Europe’s leading healthcare provider, include United Drug, LloydsPharmacy, and TCP Homecare. The group were delighted to announce that they have been shortlisted for the Health & Safety Excellence Awards 2023 under the categories of Healthcare and Warehousing.

The Healthcare Group began their discussions back in 2020 around the potential dangers of Covid-19 to the business. It was critical that whatever challenges lay ahead, would not impact the supply of vital medicines across the Irish Healthcare system and that every Pharmacy and distribution site would, where possible, remain operational.
Today, the Covid-19 task force remains active alongside their teams who maintain Ireland’s sole distribution for the vaccines. The priority remains, to protect employees whilst also meeting customer and patients’ needs and ultimately ensuring that the supply chain for the requirements of Pharmacies and Hospitals across Ireland is not impacted by Covid-19.
Best of luck to our Health and Safety teams and all those who contributed to the Covid-19 Task force.
Cosmetic Association Trade Show
The Cosmetic Association is very excited to be back in RDS again in May 2023 because their return last year, after the two-year absence, was very successful. They had our event only two months into resumption of business, and it was a delight.
Commenting on the perception that medicine shortages are a result of exceptional circumstances and are a one-off situation, Ms Gannon pointed to the level of EU activity on the topic, as well as the focus of the European Medicines regulator (EMA) on medicine shortages as evidence that this problem is not going away without serious intervention and planning.
“There’s an awareness in other European countries that market related factors need to be tackled. Medicines shortages are not just winter specific, and shortages are not only occurring as a result of exceptional circumstances. There are systemic factors that need resolution.
“Each patient has different needs and reducing the problem down to exceptional circumstances alone diminishes the quality of life impact that each patient experiences with their illness.”
Cosmetic Association Trade Show
This year they are back in the Main Hall and Hall 3. There are plenty of new exhibitors and a wide range of ‘never before seen’ products at our trade show. All their exhibitors have risen to the challenge of decorating their stands to the highest level and the event will be bright, happy and welcoming.
They hope you will all be able to attend. Buyers are the only people admitted and you will have plenty of time to choose the best ranges for your particular businesses. Please check out their website www.cosmeticassociation.ie

grounds of RDS. On registration, you will receive a brochure, floor plan and a voucher for tea/coffee and a pastry. This will get you started, or give you an opportunity to take a break, during your visit.
As they have always done, your parking is paid for within the
The dates are: May 14/15/16th 2023.
The Cosmetic Association is very excited to be back in RDS again in May 2023 because our return last year, after the two-year absence, was very successful. We had our event only two months into resumption of business, and it was a delight.
This year we are back in the Main Hall and Hall 3. There are plenty of new exhibitors and a wide range of ‘never before
PHARMACYNEWSIRELAND.COM 6 News
seen’
products at our trade show. All our exhibitors
28 PACK NOW AVAILABLE. 28 PACK NOW AVAILABLE
CCF: 24971 Date of preparation: (09-22)
ABBREVIATED PRESCRIBING INFORMATION
Product Name: Emazole Control 20 mg Gastro-Resistant Tablets
Composition: Each tablet contains 20 mg esomeprazole (as magnesium dihydrate).
Description: Light pink oval lm coated tablet.
Indication(s): Proton Pump Inhibitor (PPI): Short-term treatment of re ux symptoms (e.g. heartburn and acid regurgitation) in adults. or crush. Disperse in half a glass of non-carbonated water if di culty in swallowing. Stir until tablets disintegrate, drink liquid with pellets immediately or within 15 min, or administer through a gastric tube. Do not chew or crush pellets. Adults: The recommended dose is 20 mg esomeprazole (one tablet) per day. achieve improvement of symptoms. Duration of treatment is up to 2 weeks. Once complete relief of symptoms has occurred, treatment should be discontinued. If no symptom relief is obtained within 2 weeks of continuous treatment, the patient should be instructed to consult a doctor. recommended. No relevant use in this group in the indication: “short-term treatment of re ux symptoms (e.g., heartburn and acid regurgitation)”. Severe impaired renal function: Caution.
Severe liver impairment: 20 mg max daily dose.
Contraindications: Hypersensitivity to esomeprazole, substituted benzimidazoles or any of the excipients. Not with nel navir.
Contact a physician if symptoms change in character. In the presence of any alarm symptom (e.g. signi cant unintentional weight loss, recurrent vomiting, dysphagia, haematemesis or melaena) and when gastric ulcer is suspected or present, malignancy should be excluded, as treatment with esomeprazole may alleviate symptoms and delay diagnosis. Treatment with proton pump inhibitors (PPIs) may lead to a slightly increased risk of gastrointestinal infections such as Salmonella and Campylobacter and in hospitalised patients, also possibly Clostridium di cile. Patients should consult their doctor before taking this medicinal product if they are due to have an endoscopy or urea breath test. Absorption of vitamin B12 may be reduced due to hypo- or achlorhydria. Not recommended for long-term use as the following may also occur: Hypomagnesaemia; Risk of fracture. Consider stopping Emazole Control in cases of Subacute cutaneous lupus erythematosus (SCLE) accompanied by arthralgia. Interference with laboratory tests: Increased Chromogranin A (CgA) level may interfere with investigations for neuroendocrine tumours. To avoid this interference, Emazole Control treatment should be stopped for at least 5 days before CgA measurements. If CgA and gastrin levels have not returned to reference range after initial measurement, measurements should be repeated 14 days after cessation of PPI treatment. Contains glucose and sucrose.

Interactions: E ect of esomeprazole on other drugs: Co-administration with atazanavir is not recommended. If the combination of atazanavir with a PPI is judged unavoidable, close clinical monitoring is recommended in combination with an increase in the dose of atazanavir to 400 mg with 100 mg of ritonavir; esomeprazole 20 mg should not be exceeded. Esomeprazole is a CYP2C19 inhibitor. When starting or ending treatment with esomeprazole, the potential for interactions with drugs metabolised through CYP2C19 should be considered. Serum levels of cilostazol, cisapride, tacrolimus, methotrexate may be increased. An interaction is observed between clopidogrel and esomeprazole, but the clinical relevance is uncertain. As a precaution, concomitant use of esomeprazole and clopidogrel should be discouraged. Gastric acid suppression by PPIs increase or decrease absorption of drugs with pH dependent absorption (decreased absorption of ketoconazole, itraconazole); esomeprazole inhibits CYP2C19 metabolising enzyme and could increase plasma concentrations of diazepam, citalopram, imipramine, clomipramine, phenytoin (monitor plasma levels of phenytoin), etc. resulting in need of a dose reduction; monitor INR when given with warfarin or similar. Caution as absorption of digoxin can increase. E ect of other drugs on esomeprazole: CYP2C19 and CYP3A4 inhibitors (clarithromycin, voriconazole) may increase the esomeprazole exposure. Dose adjustment not regularly required, except in severe hepatic impairment and long-term use. CYP2C19 and/or CYP3A4 inducers (rifampicin and St. John’s wort) may lead to decreased esomeprazole serum levels by increasing the esomeprazole metabolism.
Pregnancy and Lactation: Caution in pregnancy due to lack of clinical data. No studies in lactating women, therefore, not recommended during breast-feeding. Ability to Drive and Use Machinery: Minor in uence on the ability to drive or use machines. Adverse reactions such as dizziness (uncommon) and blurred vision (rare) have been reported. If a ected, patients should not drive or use machines. Undesirable E ects: Common: Headache, abdominal pain, constipation, diarrhoea, atulence, nausea/vomiting, fundic gland polyps (benign). Uncommon: Peripheral oedema, insomnia, dizziness, paraesthesia, somnolence, vertigo, dry mouth, increased liver enzymes, dermatitis, pruritis, rash, urticaria, fracture of the hip, wrist or spine. For other side e ects refer to the SPC.
Marketing Authorisation Holder: IQ Pharmatek Ltd., Gurtna eur, Old Waterford Road, Clonmel, Co. Tipperary. Marketing Authorisation Number: PA 22777/001/001. Further information and SPC are available from: Rowex Ltd, Bantry, Co. Cork. Freephone: 1800 304 400 Fax: 027 50417. E-mail: rowex@rowa-pharma.ie
Legal Category: Not subject to medical prescription.
Date of Preparation: September 2019
Adverse events should be reported. Reporting forms and information can be found on the HPRA website (www.hpra.ie) or by emailing medsafety@hpra.ie or by emailing Rowex pv@rowa-pharma.ie
Through Pharmacy
Supply
Only
Sharing Visions in Stroke Care
The first in-person conference to focus on ‘The vision for a comprehensive stroke care pathway in Ireland’ was hosted by the iPASTAR (Improving Pathways for Acute Stroke and Rehabilitation) programme at the RCSI Education and Research Centre, Beaumont Hospital.
Ian Carter, CEO, RCSI Hospital’s Group; Prof. Fergal O’Brien, Deputy Vice Chancellor for Research and Innovation, RCSI; Prof. Frances Horgan, Profesith

Public consultation launched by PSI
The Pharmaceutical Society of Ireland (PSI), the pharmacy regulator has commenced a public consultation on a proposal to amend the statutory rules underpinning the regulator’s registration requirements.
It is part of efforts to facilitate a change to the process pertaining to pharmacist applicants from countries outside of the European Union and European Economic Area.
co-designed approach that iPASTAR aims to achieve. Bringing clinicians, academics and patients together to address the challenges and opportunities in stroke care will enable us to make positive, evidence-based changes, optimising the patient pathway.”
As the regulatory body responsible for ensuring patient and public trust in the provision of pharmacy care and services, the PSI oversees the registration of over 7,050 pharmacists and almost 2,000 pharmacies.
iPASTAR is a collaborative doctoral training award funded by the Health Research Board Collaborative Doctoral Awards Programme, and hosted by RCSI and UCD.
The conference brought together healthcare professionals, academics, Public and Patient Involvement (PPI) partners and key stakeholders to celebrate the European Stroke Organisation (ESO) accreditation of the Stroke Service at Beaumont Hospital as a comprehensive stroke centre
and present iPASTAR team’s vision for comprehensive stroke care pathway in Ireland.
The new Beaumont stroke unit is the first in Ireland and the UK to be awarded the prestigious ESO accreditation.
Commenting on the success of the event, Professor Frances Horgan, iPASTAR lead and Professor at the School of Physiotherapy, RCSI, said, “The discussions at the symposium today have encompassed the collaborative,
Date for your Diary
RCSI Centre for Professionalism in Medicine and Health Sciences, supported by the Bon Secours Health System (Lead Sponsor) and Medical Protection Society are delighted to announce the date for their annual conference:
Professionalism: The Cost of Caring
Join them on the 28th April 2023 for a day of exciting talks and presentations.
A ‘design sprint’ workshop preceded the conference where participants heard from the PPI partners in the project, including the perspectives from a stroke survivor on their experience of life after stroke and being involved in iPASTAR and discussed an ‘ideal’ stroke pathway, from acute care, transition to home to living well and healthy after stroke.
During the symposium, iPASTAR PhD research scholars Dr Deirdre McCartan, Geraldine O’Callaghan, Patricia Hall and Clare Fitzgerald presented an update on their PhD projects, which focus on delivery of integrated stroke care for patients, from the hospital, to rehabilitation in the community, and living well after stroke.
The existing route for nonEuropean Union and European Economic Area applicants to gain qualification recognition, commonly referred to as the Third Country Qualification Recognition (TCQR) route, is a multi-stage process in place since 2009. A new policy approach by the pharmacy regulator has identified the need to make changes to the route with the intention of streamlining the process, benefiting both applicants, the regulator and the wider public.
This year they are delighted to host a hybrid (online and in person) event which gives you the opportunity to participate and engage with our conference, no matter where you are in the world.
The event focuses on Medical Professionalism and promises to be a great day of exciting talks and presentations from an international panel of speakers from Canada, USA, Australia, UK, UAE and Ireland! Joined by colleagues such as Johanna Westbrook from University of Sydney, Colin West from the Mayo Clinic and Yvonne Steinert from McGill, Dr Henry Marsh of “Do No Harm” fame, amongst many others.
Registration for the online event is FREE!
Please note there is a nominal fee to attend in person 5 CPD points.
Registration Link - https://bit.ly/MedProf23Registration
Put the date in your diary and register now.
Don’t forget to follow on Twitter and use #MedProf23
As the current qualification recognition and registration processes are based in statutory rules, they now require revision and approval in order to enable the progress of these proposed policy changes. It is hoped that revisions to the TCQR process would be in place by year-end. Consultation details can be found on the PSI website and participants can provide feedback to the PSI either by completing a short feedback survey, by email to consultation@ psi.ie or by making a submission to the PSI by post. The deadline for receipt of responses is 19 March 2023.
The ongoing work by the pharmacy regulator is taking place as numbers on the register of pharmacists, and applicant numbers, continue to rise, returning to pre-pandemic levels.
The draft Registration Rules and details on the public consultation, are available on the PSI website, www.psi.ie.
PHARMACYNEWSIRELAND.COM 8 News



P R OT ECTI O N W I T H O U T C O M P R O M I S E
OUR PROVEN PROTECTION All Riemann P20 products deliver broad spectrum UVA and UVB protection that is photostable guaranteeing a durable sun protection for you and your family. Sun Facts Enlighten yourself at P20.com
YOUR MAGIC MOMENTS
Experts Call for National Life Sciences Strategy to Improve Irish Patient Care

Panel of Guaranteed Irish pharmaceutical experts call on Government and key stakeholders to collaborate to achieve more timely access to medicines for Irish patients.
Future Industry Opportunities
The Annual Guaranteed Irish Pharmaceutical Forum, hosted by Guaranteed Irish featured an industry leading line-up within the pharmaceutical sector. The panel discussion featured industry thought leaders Mairead McCaul

Managing Director of MSD Ireland
Human Health, Matt Moran Director of BioPharmaChem Ireland, Ibec, Brenda Dooley CEO AXIS Consulting and Michael
O’Connell Country Director of Biogen and President of the Irish Pharmaceutical Healthcare Association (IPHA). The attendees included more than 100 registrations from pharmaceutical businesses across the country.
Industry Successes to Date
The panel outlined Ireland’s position as a major global player in pharmaceutical production, employing over 30,000 people in Ireland directly, and a further 30,000 indirectly, with Irish exports exceeding ¤100 billion. Ireland is now the largest net exporter of pharmaceuticals in the EU accounting for over 50% of all exports from the country and is one of the main hubs of manufacturing pharmaceuticals and biopharmaceuticals in the world, with 24 of the 25 global leaders in the industry based in Ireland.
The PMI’s Annual Pharma Summit will be held on March 30th, 2023 at Croke Park
Current Industry Challenges
While Ireland is a global leader in the pharmaceutical industry, timely access to medicines in Ireland is a concern. Periods of up to 2.5 years are the norm for full Health Technology Assessments (HTA) to be made on new medicines; much longer than in other jurisdictions such as Scotland, which is between 6 and 12 months. Resourcing, and the availability of resources to evaluate medicines is a factor in the delayed reimbursement of medicines. As we move to an era of ever-more complex medicines, innovations, Gene & Cell Therapy (GCT) and potential cures; without regular and important conversations between Government, key stakeholders and industry leaders, Ireland is likely to be left behind on the global stage, as will patients. A robust system is needed to ensure the cost effectiveness of new innovations are affordable to both the state and the consumers.
The panel of experts also highlighted the challenges facing the industry including talent retention and building a workforce for the future of pharma in Ireland, including tackling the ever-present problem of training educators to help them prepare the next generation for skillsets which may not exist yet.
The panel also discussed the need for a life sciences strategy for Government, stating that 18 of the 20 biggest life sciences manufacturers in the world operate here in Ireland, and that some of these companies in the reimbursement process are finding it difficult to get their innovations to patients in reasonable timeframes. Timely patient access to medicines should be a primary goal of any Government and Health Minister, regardless of political stance or party allegiance. As of January 2023, there is no firm life sciences strategy from Government which incorporates medicines and patient access to medicines.
Panel Call to Government
1. Timely patient access
2. Commitment to development of life sciences strategy
3. Providing additional resources to evaluate and reimburse medicines quickly

4. Attract R&D and clinical trials to Ireland as a boutique destination with experience in the pharmaceutical industry
Finally, Mairéad McCaul, Managing Director of MSD Ireland Human Health, praised Guaranteed Irish, acknowledging the role the organization plays in promoting Ireland and facilitating networking opportunities for likeminded industry experts and leaders to share ideas and create new key relationships, and position Ireland as an ideal location for further pharmaceutical investment.
The theme for the day is “Partnering to Improve Human Health” and the event will be exploring this theme throughout the day from four vantage points: Technology, Government, Cross Company and Intra Company.
The day will be highly interactive with a mix of keynote speakers and panel discussions with plenty of opportunities to catch up with industry colleagues and make new connections. Visit www.thepmi.com for further information.

PHARMACYNEWSIRELAND.COM 10
News
Michael O’Connell, Country Director, Biogen, Mairead McCaul, MSD, Michael O’Connell, IPHA, Brenda Dooley, AXIS Consulting, and Matt Moran, BioPharmaChem, shared key insight on ongoing trends in the pharmaceutical sector
DO YOUR COLD SYMPTOMS GET WORSE AT NIGHT?
Did you think of asking this question to your patients suffering from a cough and cold? A survey conducted among cold sufferers showed that 87% claim that at least one cold symptom gets worse at night.1
NO MATTER WHAT YOU RECOMMEND, YOU CAN
RELIEF OF 4 COLD SYMPTOMS2, FOR A GOOD NIGHT’S SLEEP.3 ADD
VICKS VAPORUB*

1 2 3 4
SORE THROAT BLOCKED NOSE
CONGESTION COUGH DUE TO COLDS
RELIEVES A BLOCKED NOSE UP TO 8 HOURS5
In approximately 1 minute4
vapour release

IMPROVES SLEEP QUALITY
Therapeutic vapours can work fast4 from the outside in the upper airway, whilst systemic drugs work from the inside For cold sufferers3

areas indicated (e.g. chest, back) and repeat up to 2-4 times a day as needed. Wear loose clothing to facilitate the inhalation of the vapours. Inhalation (Adults and children over 6 years): Place 1 – 2 x 5ml spoonsful as indicated into a bowl of hot (not boiling) water. Inhale the vapours for up to 10 – 15 minutes per time. Do not heat in the microwave or reheat this mixture. Children should always be supervised. Contraindications: Hypersensitivity to any of the ingredients. Do not administer to children < 2 years. Do not use as an inhalation for children < 6 years. Precautions: Patient groups with a history of airway disease or pronounced hypersensitivity of the airways / asthma should use with caution or consult doctor before use. Keep out of reach and sight of children. If symptoms persist, consult your doctor. Topical: Do not apply to broken skin, wounds or mucous membranes. Do not swallow or apply directly onto the nostrils, eyes, mouth or face. For external use only. Do not bandage tightly. Do not use with heat wrap. Inhalation: Do not use boiling water to prepare inhalations. Do not heat or re-heat the mixture in a microwave. Undesirable effects: Local effects: Redness, irritation of the skin, irritation of the eyes (by inhalation), allergic dermatitis. Irritations or allergic reactions are usually mild and occur rarely. General disorders and administration site conditions: Burns at application site – frequency not known. Systemic effects: Due to the recommended route of administration; systemic exposure is very low and undesirable effects due to systemic exposure have not been observed. Supply Status: Supply through non-pharmacy outlets and pharmacies. PA Number:
PA Holder: WICK Pharma - Zweigniederlassung der Procter & Gamble GmbH, Sulzbacher Str. 40, 65823 Schwalbach am Taunus, Germany. Text prepared: August 2020. Further information available on request.



1. Procter & Gamble. Online Consumer Survey conducted among 313 French cold sufferers in the last 12 months. Data on File 2022. 2. Vicks VapoRub SmPC Theraupetic indications. 3. Santhi N, Ramsey D, Phillipson G, Hull D, Revell VL, Dijk D-J. (2017) Efficacy of a topical aromatic rub (Vicks VapoRub®) on effects on self-reported and actigraphically assessed aspects of sleep in common cold patients. OJRD 7: 83-101. 4. Eccles, R., Jawad, M., Ramsey, D.L. and Hull, J.D. (2015) Efficacy of a Topical Aromatic Rub (Vicks VapoRub®)-Speed of Action of Subjective Nasal Cooling and Relief from Nasal Congestion. Open Journal of Respiratory Diseases, 5, 10-18. 5. Procter & Gamble. Technical Report RPS1147/44. Data on File 2010. * There are no known interactions with other medicines according to usage directions (SmPC 4.5).


®
®
“ ”
www.prl ie pgsales@prl ie +353 1 257 4650 PRL SALES ULC, Greenogue Business Park, Rathcoole, Co. Dublin Vicks Vaporub Inhalation Vapour, Ointment contains levomenthol, camphor, eucalyptus oil and turpentine oil. Indications: For the symptomatic relief of nasal catarrh and congestion, sore throat, also cough due to colds. Dosage and Method of Administration: Topical (Adults and children over 2 years): Rub the indicated amount onto the
PA2294/003/001
New President calls for greater role for Optometrists in public eye-care
Optometry Ireland has announced a new President – who stated her commitment to achieving better eye care for children in Ireland.
The new Optometry Ireland (OI) President is Tania Constable, a specialist in children’s eye-care who has been working within the HSE (and CHI@Temple street) for the last five years.
Beginning her tenure Tania Constable thanked outgoing OI President John Weldon for an excellent service to eye health and fellow professionals, particularly during the difficult Covid-19 period.
“I am delighted to have the opportunity to lead OI into what promises to be a period of dynamic change in the profession. Optometry can provide a key role in addressing the pressures facing the health system now and into the future.
“The first issue that needs to be addressed is access to public eye care for children, particularly for 8-16 year olds for whom there is no national public scheme.
Optometry Ireland has long raised the issue of the lack of a national scheme for the provision of public eye care for children.
“Optometrists are trained, have the required equipment and are available to provide a public programme to older children to improve their health outcomes. We can alleviate unacceptable waiting times and unsustainable pressure on hospital eye departments and GPs.”
Ms. Constable graduated from Manchester University in 2007 and worked in the UK for a number of years before returning to Ireland in 2012. She has worked in a number of different practice settings including multiples, independents and as a locum before starting her current role as a paediatric specialist within the HSE. She completed an MSc in Clinical Optometry in 2021.
She is being accompanied by a new Vice President at Optometry Ireland, Sinéad Ryan who is qualified in both Optometry and Pharmacy. Sinead has over fifteen years of practical experience working in hospital, community and academic roles in both the UK and Ireland.
Optometry Ireland CEO Seán McCrave welcomed both Tania and Sinéad into their new roles: “I am confident that Tania assisted by Sinéad will bring strong initiative. They both bring new experiences and energy to their roles.
“There are opportunities for Optometrists to provide needed capacity to the health system and they are both focused on progressing this. Both I and our Council will work closely with them to achieve better eye-health for the population aided by a thriving Optometry profession.
Bubbles, Bites and Beauty secrets
It was an evening of skincare, beauty and wellness, with a panel of speakers

Dr Hauschka expert and holistic therapist Tara O’Rourke, beauty therapist and beauty editor Triona McCarthy, CIBTAC skincare consultant & Beauty Blogger Sally Foran, and hosted by Bianca Luykx, editor of VIP Magazine. The panel discussed the latest and greatest in wellness, beauty and skincare and revealed their top beauty secrets.
Stroke Research
There has been an alarming decline in the number of stroke patients getting to hospital on time for effective stroke treatment highlighting the importance of stroke awareness campaigns.
According to the Irish National Audit of Stroke National Report: A critical review of national stroke data for Ireland from 2013 to 2021 by the National Office of Clinical Audit (NOCA), the proportion of stroke patients who arrived at hospital within three hours of the onset of their stroke symptoms decreased from 59 per cent in 2013 to 46 per cent on 2021.
The report was launched by Professor Joe Harbison, Clinical Lead on the Irish National Audit of Stroke (INAS).
In order to raise awareness of the signs of stroke and the importance of calling an ambulance as soon as possible, the Irish Heart Foundation launched a new F.A.S.T. stroke campaign.
The NOCA report also found that 73 per cent of patients got to hospital within the crucial 4.5hour window for effective stroke treatment in 2014; however, this figure had dramatically reduced to just 58 per cent in 2021.
Guests were treated to an exclusive Goodie bag worth of ¤50, and spot prizes from Benefit makeup and Dr Hauschka. Along with complimentary Kylie Minogue wine, Lindt chocolate and canapes on arrival.
Over ¤3,000 was raised in aid of fantastic Irish charity, Look Good
Feel Better. Look Good Feel Better put smiles on the faces of women receiving cancer treatment with skincare and make up workshops that give tips, techniques and a treat to those who need it.
Their mission is to help improve the well being and confidence of women undergoing treatment
Tara O’Rourke,
beauty therapist and beauty editor Triona McCarthy, CIBTAC skincare consultant & Beauty Blogger Sally Foran, and Bianca Luykx, editor of VIP Magazine
According to the data, the proportion of patients with a stroke who were seen by a medical team within 10 minutes of arrival at the hospital has more than doubled between 2016 and 2021, from 23 per cent to 48 per cent, suggesting that stroke patients can be assured of immediate attention on arriving at the Emergency Department.
for any type of cancer. They do this by providing free Look Good Feel Better workshops they can’t happen without the support of brands like Dr Hauschka.
The Dr Hauschka brand offers a range of natural skin care and beauty products. Their products utilise the healing and therapeutic properties of nature to restore and maintain healthy skin. The company is dedicated to protecting and preserving the environment and has as an ethos underpinned by ecofriendly principles.
The report also found that the proportion of patients who had brain scan within 1 hour of arrival at hospital increased from 20 per cent in 2013 to 48 per cent in 2021. However, for those who were treated with thrombolysis, the proportion who received it within 60 minutes of arrival at hospital increased considerably, from 25 per cent in 2013 to 56 per cent in 2021.
PHARMACYNEWSIRELAND.COM 12 News


www.theapharma.ie Europe’s No 1 dry eye drops Hydrates & Lubricates Repairs & Protects Lasts for up to 4 hours Clinically Proven1 to treat symptoms of dry eyes Available on the GMS Action 2 1 Pinto-Bonilla JC et al. Ther. Clin Risk Manag 2015:11;595-603 2 IQVIA MAT September 2022 Ireland Dry Eyes
A Pathway to Success!
SuperIntendent Pharmacist Ronan Ward talks to us about his career progression
My name is Ronan Ward and I am a Superintendent Pharmacist with McGreals Pharmacy Group, a position I have held for the last 3 years.

What motivated you to pursue a career in Pharmacy?
I always had an interest in science and so always felt I would follow a career related to that. Occupations such as pharmacy, optometry, physiotherapy amongst others were all possibilities, but as a teenager that is a tough decision to make as I’m sure we all remember. The swinging vote was probably that my older brother had just qualified as a pharmacist and was already driving round in a nice car, going on nice holidays and I thought if he can have all that then heck so can I! I’m not sure that is really the best way to decide your future career but I did anyway and happily it all worked out for me.
Can you tell us about your career progression and what led you to become Superintendent Pharmacist at McGreals Group?

thing. Having explored different opportunities, a meeting with Kilian McGreal, CEO of the McGreals group, was the one that grabbed my attention. Immediately I got a different vibe from Kilian and the group, and was delighted to take up a Supervising pharmacist role. After a period of time the role of Superintendent Pharmacist was brought up, Kilian had been performing the role but with a full schedule as CEO of a developing company he was looking to relinquish it. This really felt like one of the few opportunities pharmacists have to progress so I applied and for better or worse took on the mantle. With a good few years experience behind me and having had a good role model in the form of the Superintendent from my previous group, I felt I was in a good place to take it on.
Do you enjoy working as a Pharmacist and why?
After qualifying, and working for a large multinational in the UK for a short while I decided that it was time to return to Ireland. I fortunately obtained a pharmacist position with a relatively large Irish owned pharmacy group and after a period of time progressed from relief pharmacist to Supervising Pharmacist and maintained that position for approximately 10 years. With thoughts of some kind of career progression, and the arrival of little feet to which long shifts and late nights do not necessarily suit, I decided that a move might be a good
Admittedly it is a challenge and brings its own pressures but it can be rewarding and certainly adds a new dynamic to the working day, boredom is not something I have an issue with! I have to admit that the pharmacists, and support technicians, we have in the group are brilliant and they make my job a lot easier. Professional, great with their patients and able to use their own initiative all takes a lot of pressure off the Superintendent role. Sure, they don’t break into massive smiles every time I bring round a new suite of SOPs, but they perform their roles to the highest of standards.
As the most accessible healthcare professional out there, the role becomes integral to the communities that we serve, and this makes the job so rewarding. We get the opportunity to work with patients directly on a daily basis and make a significant difference to their lives. Sure no-one working regularly in community pharmacy will say that there isn’t an element of repetition and same old same old in the job and in reality that is the role which we have signed up for. However as the saying goes it is one of those jobs you get out of it what you put into it. There is rarely a day you don’t pick up something new and with
not have access to this level of support and expertise and this is why, for me anyway, the partnership is a great fit.
the opportunity to engage with so many people on a day to day basis it’s a job that can be challenging, interesting and satisfying. What would you say to a Pharmacist considering a career with McGreals Group?
When I started out as a pharmacist I, like many others, had aspirations of owning my own pharmacy but as time went by the challenge of capital and feasible opportunities made that increasingly difficult. After joining the McGreals group and having settled into the company it was made clear to me by Kilian that they valued me as a part of the group and would extend the offer of part ownership to me based on the right opportunity for both parties coming up. Several projects were looked at but when the pharmacy at Glenageary came up all parties felt that this was definitely a project that worked for everyone. Whilst for some full ownership of a business is what they really desire for me, personally, having the support of the group is invaluable. Whilst I don’t own the pharmacy outright it feels like the pharmacy, and all the related decisions and running is effectively mine. With that I have all the backing and support of the McGreals Group office including HR, finance, payroll, property services and a fantastic Marketing team. As an independent operator you would not have access to this level of support and expertise and this is why, for me anyway, the partnership is a great fit.
A Pathway to Success!
PHARMACYNEWSIRELAND.COM 14 News
SuperIntendent Pharmacist Ronan Ward talks to us about his career progression
Also suitable for babies who may be prone to eczema



1
Cleanse gently without damaging skin barrier

2

Moisturise to instantly soothe dry, itchy skin
3



Long-lasting comfort at night, clinically proven to relieve itchy sensation

Clinically proven to help moisturise & soothe baby’s dry, itchy skin.
IE-AVB-2200061
Baby Focus: Skin
A Softer Touch – Pharmacy Guide to Baby Skincare

Babies are a customers most prized possession, and therefore any signs of in their child can be worrying – and their concern is not helped by the alarmist information that can be found on the internet. One of the most important things pharmacy teams can do is provide reassurance.
common, harmless condition that does not usually itch or cause any discomfort to the baby.
Cradle cap usually begins in babies during their first three months and tends to last a few weeks or months. It usually clears up by the time the child is two years old, although in rare cases children can have cradle cap for a lot longer.
The cause of cradle cap is not clear, although it may be linked to overactive sebaceous glands, which are glands in the skin that produce an oily substance called sebum.
Pharmacists can advise that cradle cap requires no specific treatment, although gently washing the baby’s hair and scalp may prevent a buildup of the scale.
Chickenpox
Symptoms include a rash made up of tiny spots, bumps or sometimes blisters, surrounded by a patch of red skin. The symptoms can be accompanied by mild swelling, itching, and a stinging or prickling sensation. It is commonly found on the face, back, neck, chest and thighs. Treatments include hydrocortisone cream (but not to the face), calamine lotion, antihistamines (where appropriate); wearing cotton clothing, avoiding excessive heat and humidity, and keeping skin cool.
Advise parents to call a health professional urgently if a rash does not fade when the skin is pressed with the side of a glass.
Nappy rash
Eczema
Atopic eczema is a very common skin condition, affecting one in five children. Atopic dermatitis is the most common form of eczema affecting young children. For most children affected, the disease is mild. However, often those who have seemingly outgrown the condition will continue to have lifelong sensitive skin and may have recurrences of eczema following long symptom-free spells.
An intense itch is the major symptom of atopic eczema. Scratching only provides momentary relief, and leads to more itching (the itch-scratch cycle). Scratching worsens eczema and can make the skin more vulnerable to infection. The intense itch is very uncomfortable, can disrupt sleep and negatively impact on the child’s quality of life, as well as that of his/her parents and the wider family. Some children with more pronounced eczema can also experience social embarrassment due to the visibility of their condition.
In infancy, the first noticeable signs of atopic eczema may be skin dryness and roughness, but

other symptoms (e.g. red itchy skin which can affect the cheeks and forehead, and/or the trunk and outer aspects of arms and legs) do not usually occur before two months of age.
In older children, from about 1-2 years onwards, atopic eczema is most often seen on the inner sides of the arms at the elbow creases, behind the knees, and on the face and neck.
Emollients can be used for daily use on dry skin – including bath soap substitutes that are free of sodium lauryl sulphate; topical corticosteroids during flareups. Advise parents to try and encourage their child not to scratch and help them avoid triggers.
Recommend a GP if you notice very red and weepy eczema with small blisters, as this could signal an infection. Similarly, if the skin is cracked or the problem is persistent or worsening.
Cradle Cap
Cradle cap is the name given to the yellowish, greasy scaly patches that appear on the scalp of young babies. It is a very
Also known as varicella zoster virus, chickenpox is often seen in children under eight years of age. Symptoms include an itchy rash (mainly on the chest and back) comprising of spots that resemble blisters. Discomfort is notably worse if the skin is too warm.
Chickenpox tends to last between 7-21 days. Paracetamol should be given in the case of fever and cooler baths. Calamine lotion is the traditional option for topical use but is drying in nature. Newer cooling gels/sprays are available to reduce itching and limit any potential scarring.
Advise parents to keep their child away from others –especially pregnant women or immunosuppressed individuals. Ibuprofen is no longer advocated as it can make the lesions worse.
Recommend a GP if the child appears to be very unwell.
Prickly heat
Prickly heat is a skin irritation that occurs when the sweat glands are blocked. Babies and children are more at risk because of their under-developed sweat glands.
Dermatitis on babies’ bottoms is very common, and can be very painful. It is usually due to occlusion and irritation from dirty or wet nappies. Less commonly it can be caused by candidiasis or psoriasis. Rarely it can be caused by irritation or allergies to products used to clean the area.
When parents present to the pharmacy for advice for nappy rash, good recommendations would include the use of a barrier cream, use of hypoallergenic water wipes, nappy-free time, and more frequent nappy changes. If these measures fail to improve the nappy rash, a topical antifungal agent such as miconazole cream could be considered, with early review by a doctor if this fails to resolve the dermatitis.
Facial rashes in newborn babies
Babies can develop multiple red/ white spots, with an appearance of mild ‘acne’ (neonatal cephalic pustulosis) in the first month that is harmless and goes away without treatment. Small white spots on the nose, forehead, or cheeks (called sebaceous hyperplasia) resolve over a few weeks.
When parents present to the pharmacy with these issues, the best advice is to await spontaneous resolution over the coming weeks.
16 | PHARMACYNEWSIRELAND.COM






For topical use only. Cleanse and dry the affected area before applying. A copy of the summary of product characteristics is available upon request. The active ingredient in Caldesene Medicated Powder is Calcium Undecylenate 10% w/w, 20g, 55g, 100g pack size. PA 126/152/1 PA Holder: Clonmel Healthcare Ltd., Waterford Road, Clonmel, Co. Tipperary. Date Prepared: October 2022. 2022/ADV/CAL/283H TENDER CARE AT Every Change Caldesene prevents and treats nappy rash. Born in 1977. Still No.1 in Ireland*. *as voted by the readers of mums & tots.
Baby Focus: RSV
Respiratory Syncytial Virus: An Overview
Respiratory syncytial virus (RSV) is a common, ubiquitous and contagious viral pathogen that infects the respiratory tract of most children by 2 years of age.
majority of deaths are in resourcelimited countries.”
We recently spoke to Theresa Lowry Lehnen, Clinical Nurse Practitioner and Associate Lecturer South East Technological University to find out more about the condition.

RSV is an RNA pneumovirus of the Paramyxoviridae family, and humans are the only natural host. Theresa explains, “RSV typically spreads via hands, fomites and the airborne aerosol route. Respiratory syncytial virus spreads from person to person by aerosol droplets through coughing or sneezing, and is also spread through direct contact by touch.”
Respiratory syncytial virus is primarily a childhood infection, however, it may occur at any age and can be most severe in infants under one year of age, the immunocompromised, and in people aged 65 years and older, she says.
“It infects 90% of children within the first 2 years of life and frequently re-infects older children and adults. Respiratory Syncytial Virus infection can present as a variety of clinical syndromes including upper respiratory tract infections, bronchiolitis, pneumonia, exacerbations of asthma and viral-induced wheeze.
“Worldwide, it is estimated that RSV is responsible for approximately 33 million lower respiratory tract illnesses, three million hospitalisations, and up to 199,000 childhood deaths. The
Respiratory Syncytial Virus infection has been a notifiable disease in Ireland since January 2012, and RSV activity in Ireland is monitored by the HSE-Health Protection Surveillance Centre (HPSC). RSV notifications are reported in the HPSC infectious disease weekly report and outbreaks in the weekly outbreak report. According to the HPSC (2022), nearly all children have been infected with RSV at least once, by two years of age.
Theresa adds, “Most cases are not specifically diagnosed as RSV, however, the infection causes 80% of bronchiolitis and 20% of pneumonia cases in young children and RSV is a significant cause of infection and outbreaks in hospitals, neonatal units, day units and nursing homes.
“While most infections cause only mild symptoms, RSV is the most important cause of viral lower respiratory tract infection (LRTI) in infants and children globally, and is responsible for one-third of deaths resulting from acute LRTI in the first year of life. In medium and high resource countries, RSV mortality rate in infants is almost nine times that of influenza.
“Respiratory Syncytial Virus infections occur in a seasonal pattern in temperate climates with epidemics from October to April. Outbreaks typically occur in the winter months with the highest numbers of infections usually reported in December and January every year.
There is only one serotype of RSV, but it is classified into two strains, “A” and “B,” with differences consisting of variation in the structure of several structural membrane proteins, most especially the attachment protein. One of the two major antigenic subgroups of RSV A or B, usually predominates each season.
Transmission occurs through contact with aerosolised viral particles generated through sneezing and coughing, or from contaminated surfaces or fomites. She adds, “Largeparticle droplets can survive on contaminated surfaces for up to 6 hours. Handwashing is the most effective infection control procedure. Infected individuals shed RSV for 3 to 8 days but immunocompromised patients with severe infection may shed virus for up to 4 weeks.
“The frequent occurrence of mild or asymptomatic infection in otherwise healthy individuals makes infection control challenging. Incubation
Period and Symptoms The incubation period for RSV is usually 4 - 6 days, but ranges from 2 to 8 days depending on host factors such as the age of the patient and whether it is the patient’s primary infection with RSV.
“After inoculation into the nasopharyngeal or conjunctival mucosa, the virus rapidly spreads into the respiratory tract, where it targets its preferred growth medium, apical ciliated epithelial cells. There it binds to cellular receptors using the RSV-G glycoprotein and uses the RSV-F fusion glycoprotein to fuse with host cell membranes and insert its nucleocapsid into the host cell to begin its intracellular replication.”
Symptoms of RSV include; fever, rhinorrhoea, pharyngitis, nasal congestion, sneezing, coughing which can be croupy or barking in nature, tachypnoea, sore throat, wheeze, decreased appetite and ear infections in children. In very young infants, irritability, decreased activity and breathing difficulties may be the only symptoms of infection. Lower respiratory tract infections, such as pneumonia or pneumonitis, are most likely to occur during a child’s first infection with RSV and may develop in 3070% of first infection.
Typically, only between 1% and 3% of infected infants require hospitalisation.
“The infectious period lasts from shortly before onset to one week post the onset of symptoms. Most children recover in 8- 15 days,” Theresa notes. “Even after recovery,
however, very young infants and children with weakened immune systems can continue to spread the virus for 1-3 weeks. Immunity is incomplete and short-lived.”
Bronchiolitis is an inflammatory process in the small airways of the lungs and is the most common clinical syndrome associated with RSV infection. It typically presents in infants under 1 year of age but may be diagnosed in children up to 2 years old, and is characterised by a short history of low-grade fever, cough, coryza, dyspnoea and reduced feeding. The symptoms usually peak in clinical severity between day 3 and 5 of the illness.
“RSV bronchiolitis presents a significant clinical burden,” Theresa tells us. “In the UK, infection with RSV is responsible for up to 80% of all cases of bronchiolitis, similar to that of 65–70% in the US. In older children, Respiratory Syncytial Virus typically presents as an URTI, viral pneumonia, episodic viral-induced wheeze or an acute exacerbation of asthma.”
Viral pneumonia is a common illness with 5 million cases reported in children annually. A meta-analysis of nine studies involving over 4000 children investigating viruses identified by polymerase chain reaction, found that RSV was the causative organism in 11% of communityacquired pneumonia cases.
Theresa says that diagnosis includes a thorough medical history and a physical exam. “A chest X-ray may be requested and blood and urine tests may be carried out to out-rule a bacterial infection or other conditions. Differential diagnosis can include, asthma, bronchiolitis, influenza, croup, bronchitis and pneumonia.
“Respiratory viral testing may be used in a clinical setting to increase confidence in the diagnosis of a viral, rather than bacterial, cause for respiratory illness. RSV can be detected in nasopharyngeal aspirate, broncho-alveolar lavage, sputum, or swabs from the nose and throat by using real-time PCR, immunofluorescence, ELISA and growth in cell culture. Reverse transcriptase-polymerase chain
18 | PHARMACYNEWSIRELAND.COM
An interview with Theresa LowryLehnen (PhD), CNS, GPN, RNP, South East Technological University





the
Calpol ® Vapour Plug & Nightlight (from 3 months) to help with clear and easy breathing. Non medicine. Always read the label. IE-CAR-2300006
Available in 5’s & 10’s NEW Orange Light for a more restful sleep
Recommend
Calpol Vapour Plug for clear and easy breathing through the night
Refills
Baby Focus: RSV
reaction (RT-PCR) assays are currently the gold standard in RSV testing and are available commercially. These are more sensitive than antigen detection and virus isolation methods,” she adds. The mainstay of treatment for the vast majority of RSV infections is supportive including rest, fluids and paracetamol, but passive preventive immunisation is available for at-risk children, including premature infants and infants with a history of cardiac, pulmonary, or neuromuscular diseases.
“Those with severe respiratory illness require hospitalisation, oxygen therapy, IV fluids and ventilatory support in the form of a high-flow nasal cannula, CPAP, or intubation, and mechanical ventilation. Ribavirin is the only licensed antiviral medication for the specific treatment of RSV infection but due to drug toxicity, including bone marrow suppression and potential carcinogenicity and teratogenicity and minimal clinical benefit, it has not been recommended for routine clinical use.
“Ribavirin, may be considered for a small number of patients and treatment of RSV with Ribavirin must be done under the supervision of an infection specialist such as a consultant microbiologist or an infectious disease specialist. Other treatment
modalities for bronchiolitis have been tried in the past and have failed to show broad, reproducible efficacy on clinically significant outcomes in RSV and bronchiolitis. Antibiotics are not effective against RSV and it is important that unnecessary antibiotics are discontinued once a diagnosis is confirmed, to avoid adverse drug reactions and antibiotic resistance.
“Infants who are recovering from RSV bronchiolitis can continue to have respiratory symptoms including cough and postbronchiolitis wheeze for several weeks/months. There is no evidence for the use of steroids, montelukast or other medications in preventing these symptoms but the acute episodes often respond to anti-asthma medication.”
Theresa notes that high-risk infants with other co-morbidities may require longer admission and some may even require mechanical ventilation.
However, she adds, “the majority of children with RSV make a full recovery and have an excellent outcome. The majority of children who need hospital admission are usually discharged in several days. Some infants with RSV may develop wheezing but recent studies do not show an increased risk of asthma. Prevention and patient education is key, and frequent, careful handwashing is
the most important measure in preventing the spread of RSV.
“Respiratory etiquette should be properly maintained and people with cold/flu-like symptoms should cover their nose and mouth preferably with a tissue or cough and sneeze into their elbow and wash their hands afterwards for at least 20 seconds or use an alcohol-based rub/gel. Used tissues should be properly disposed of.
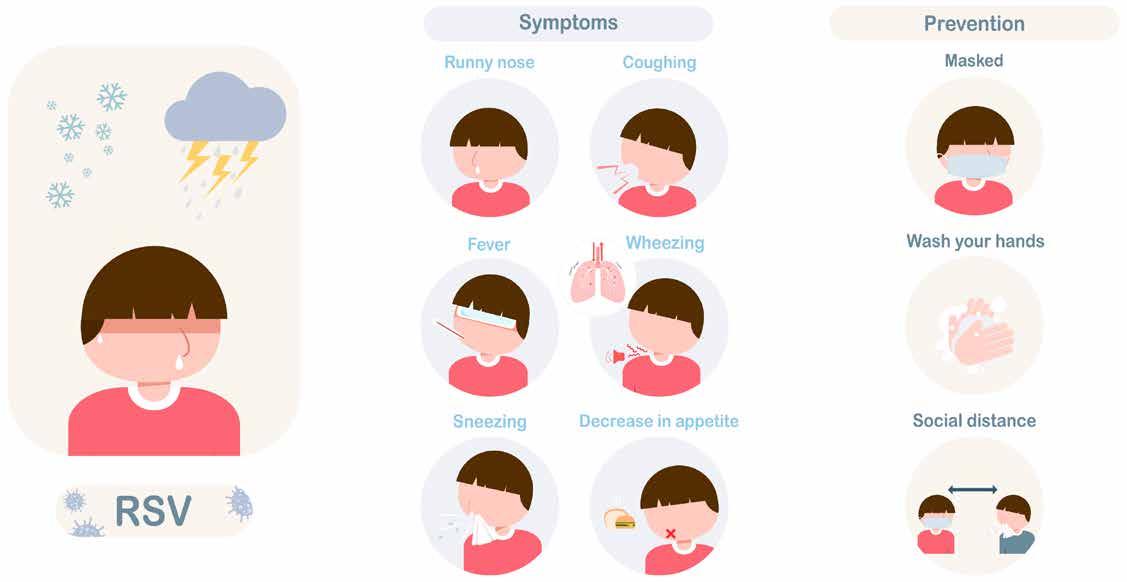
“Sharing utensils with persons who have RSV illness should be avoided and cleaning contaminated surfaces such as door handles may help stop the spread of RSV. Parental smoking is a known risk factor for RSV infection in infancy, and parents or carers who smoke should be offered smoking cessation advice and encouraged to stop smoking. Breastfeeding also offers some protection against RSV infection.
“Persons with RSV should not attend crèches, school, work and non-residential institutions until well. It is important to prevent young infants, frail older persons and immunocompromised people coming into contact with individuals with respiratory infection.”
The management of Respiratory Syncytial Virus disease in infants and children is primarily supportive with antiviral medications reserved for the most vulnerable, she
concludes. “The development of a well-tolerated, clinically effective and cost-effective RSV vaccine and therapeutic agent remains a global health priority. It is likely that a licensed RSV vaccine is several years away, however, given the burden of RSV infection and the associated costs globally there is much ongoing research into the development of a well-tolerated and effective vaccine.
“The main target populations for vaccination include infants, school age children, pregnant women and older adults. At least 14 anti-RSV treatment products are undergoing phase I and II clinical trials, of which 5 have included paediatric patients. Novel therapeutic molecules developed to date include, fusion inhibitors, non-fusion inhibitors, polymerase inhibitors, antibodies, nucleoside analogues, small-interfacing RNAs and a benzodiazepine. They have various targets on RSV such as the F protein, RNA polymerase, nucleoprotein and nucleocapsid mRNA. It is hoped that one of these products will become a licensed treatment for RSV infection in children and adults over the coming years.
“The development of a successful treatment or prophylactic agent has the potential to revolutionise the care and outcome for severe RSV infections in the world’s most vulnerable infant population.”
20 | PHARMACYNEWSIRELAND.COM

T 1800 816 005 E info@scopehealthcare.ie W scopehealthcare.ie Contains marshmallow extract for natural cough relief! A 100% natural and preservative free cough syrup, specifically formulated for children 1 year+ for both dry and congested cough. From the makers of VIVIO® Junior Multivitamin
Stocked in wholesalers and ready for delivery. For queries or direct orders get in touch: 1800 816 005
C OU G H S Y R U P
Baby Focus: Asthma
Asthma and Inhaler Technique in Children
Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation which is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable expiratory airflow limitation (GINA, 2021)
Asthma is one of the most common chronic diseases worldwide affecting an estimated 300 million. Prevalence is increasing in many countries, especially in children. Asthma is a major cause of school and work absence (Manning et al., 2005).
The Asthma Society of Ireland estimate that that 1 in 5 children experience asthma at some stage in their life.
The goals of asthma management are:
1. Symptom control: to achieve good control of symptoms and maintain normal activity levels
2. Risk reduction: to minimize future risk of exacerbations, fixed airflow limitation and medication side-effects
Assessment of asthma control involves assessing symptoms over the previous 4 weeks and assessing risk factors for poor outcomes. Treatment issues should also be addressed at every visit and should include:
• Checking inhaler technique and adherence
• Asking about side-effects
• Reviewing the child’s written asthma action plan?
• Exploring the parent’s attitudes and goals for their asthma?
The Asthma Control Test (ACT) for children is a useful tool to
assess the child’s level of control and the impact asthma may be having on their day-to-day life (available on https://www. asthmacontroltest.com/).
Treatment
An inhaler is the most effective method of giving asthma medication as it ensures that the medication goes directly to the lungs where it’s needed, and requires smaller dosages than tablets. A spacer device is a plastic container with a mouthpiece or mask at one end, and space to insert an inhaler at the other. Spacer devices ensure the person with asthma gets the maximum benefit from their medication and helps direct it to where it’s needed in the lungs.
Children should always use a spacer with their inhaler, especially for children younger than 4.
Reliever
inhalers
Reliever inhalers relax the muscles around the breathing tubes during an asthma attack. This allows airways to open, making it easier to breathe. Most reliever inhalers are blue.
If a child needs their reliever inhaler more than 3 times a week, they will need a preventer inhaler too.
Preventer inhaler
These inhalers prevent children’s symptoms from appearing and
reduce the risk of long-term problems. Most use a small dose of steroids.
Preventer inhalers work gradually over time. They won’t relieve sudden attacks.
A child should use their preventer inhaler every day or it won’t work.
Advising Parents
Check your child’s inhaler technique
Getting the inhaler technique with their spacer or facemask right is one of the most important things parents can do to help their child stay well.
It’s very important to watch the child take their inhaler so that parents know they’ve taken it properly. It’s also important that the child’s school or nursery understand how they should be taking their inhaler.
Advise parents that they can check their child is using the right inhaler technique by:

• asking their GP or asthma nurse to check the child’s inhaler technique with their spacer or facemask at their next asthma review. It’s also important to check a child’s technique if they’re given a new type of inhaler, spacer, or facemask
• asking a pharmacist to check the child’s inhaler technique when they next pick up their child’s asthma medicines
The right inhaler technique helps you get more from your asthma medicines. It also reduces the chance of side effects and reduces wasted medicine.
Parents and care-givers should also remember to wipe the child’s face after they have used a facemask or ask them to rinse their mouth out with water after using their steroid preventer inhaler. This is to prevent side effects like thrush.
Check their child is using the right spacer or facemask
As children get bigger, the asthma inhalers, spacer, or facemask they need to use will change.
Using the right device for their size and stage of development helps them to get the full dose of their asthma medicine.
Once a child can drink through a straw, or they’re older than five, they should be using a spacer without a facemask. This is because medicine can be wasted when using a mask, as it can stick to your child’s face and to the inside of the mask.
Clean and store inhalers correctly
Cleaning and storing a child’s inhalers, spacer or facemask properly means they can work in the best way possible.
Get the child into a good routine with taking their medicine
The medicine in children’s preventer inhaler cuts the risk of asthma symptoms and a potentially life-threatening asthma attack. The protection it gives a child’s lungs builds up over time. This means children needs to take their preventer inhaler every day, as prescribed, even if they’re feeling well.
Try these top tips to help them get into a good routine:
• Putting a sticker on their toothbrush as a reminder. Research shows parents are more likely to remember to give their child their medicine every day if they link it to something they already do, such as brushing their teeth.
• Keep their preventer inhaler and spacer or facemask on their bedside table to remind them to take it when they wake up and just before going to sleep.
• Set reminders on the phone
• Ask family or friends to help remind them. This might be useful if a child has only just started using an asthma inhaler.
• Make it fun so that the child links taking their inhaler with something positive.
22 | PHARMACYNEWSIRELAND.COM

















Baby Focus: Fertility
Fertility Training for Pharmacists
With 57% of people aged 25 – 45 concerned about their fertility, research from Boots Ireland last year shone a further light on some of the key issues. Not being able to have children was the key concern experienced by 13% of respondents and this was more acutely felt among those aged 25 – 35 with 19% expressing this concern.
storage of drugs, administration, and side-effects. Drugs cost a lot and are a major investment for your customer.
“Advise them on the timing of medicines, the doses, what ‘bd and tid’ actually mean in their daily routine. Check it’s the correct medication, size, expiry dates in order, no cracks or damage to the container.
“For example, is the Gonal-F pen the correct size?
Community pharmacists have a key role to play with this particular group of patients, as the central healthcare professional within communities across Ireland.
Not being able to afford fertility treatments was listed at 12% while 11% of respondents are concerned that they might not find out about their fertility issues until it’s too late. The research also demonstrated a lack of awareness of where to go to seek advice on fertility issues.
While 72% of respondents agreed that people are starting to be more open about fertility and infertility issues, the research showed that a gender divide exists with 57% of respondents believing that the woman should shoulder most of the responsibility of fertility and family planning.
The research also investigated the impact that people’s fertility journeys have on them. Stress and anxiety is experienced by 14% of people with 13% of people saying it affected their mental health. It causes stress in relationships for 13% of people and 6% reported that their relationship ended as a result.
We spoke to Helena Tubridy to learn more about what pharmacists and their teams should consider when dealing with fertility patients.
Helena Tubridy MA RGN RN is a fertility coach and therapist who helps intending parents prepare for pregnancy, whether naturally or with ART.
Her background is in midwifery and gynae nursing, with a Master’s in Bioethics and Fertility. She also provides support and brief-therapy following miscarriage, stillbirth, and birth trauma.

Helena’s new online course is ‘Fully Charged Fertility’, a 6-part selfpaced roadmap to understanding and improving fertility to achieve pregnancy more easily and identifying any roadblocks.
Helena told us, “Community pharmacists are often the first exposure to healthcare professionals for those on the fertility journey. I always recommend my clients seek out help from, pre-conception to pregnancy and way beyond.
“Pharmacists would frequently be the first healthcare professional
I recommend, providing warmth, reassurance, expert knowledge and guidance.
“For pharmacists and pharmacy teams it is important you think about rapport building, with discretion assured, and providing support at a vulnerable time. It’s second nature to you already.
“Furthermore, don’t be afraid to engage - normalising questions about fertility supplements, the benefits of probiotics and so on. You know a lot, you thrive on accuracy, can bust myths, and help people feel less alone.
“Pharmacists should think about their ‘bedside manner’ and the placebo effect. Alia Crum’s research shows mindset around medications may even minimise side-effects.
“Customers may already have a child who was easily conceived. Secondary fertility can be perplexing and frightening. No one wants to require assistance in conceiving. It’s regarded as the most natural thing in the world for women and men. Self-confidence is eroded with feelings of failure, and self-blame.”
Helena adds that IVF drug packs can be daunting for many. They take up a lot of room in the fridge, and make it all seem quite clinical and scary. It is vital therefore, she adds, that pharmacists can teach and support these patients on ‘unboxing’ and living with their treatments.
She adds, “Customers need to know about transportation and
“Encourage these patients to consider their doses and explain why doses/schedules may vary within a cycle, or in a new cycle based on optimising hormone levels. They should be prepared for every eventuality, for example, what happens if they are away from home or travelling abroad?
“Pharmacists should also ask themselves, can you ensure a regular supply? What about responding to changes in prescription, are we as a team equipped for that?
“Consider how responsive you are in person, by phone and online. For example, are you available at weekends and during holidays or is it locum coverage? These will be important pieces of information for the patient.
“Websites can prove to be a great resource for fertility patients. One complaint I often hear is that they may not be updated or current. If you are providing information to customers within this realm then aim for brief blogs that inform.
“Injections are often a scary thought for new patients, and may need doing twice daily - so how about a good demo video on your website? Consider showing them how to prepare for an injection; Sanitisation requirements; drawing up, mixing, changing needles and administering an injectionangle and depth; taking care of the injection site and disposal of sharps.”
For updates on Instagram: Helena Tubridy
24 | PHARMACYNEWSIRELAND.COM
Helena Tubridy
Baby Focus: Gut Health The Importance of Good Gut Health in Children

The bacteria in a child’s gut plays an important role in keeping them healthy, both mentally and physically.
Gut health has become a hot topic in recent years and the discussion is usually about gut microbiome which are the trillions of bacteria that live inside our gut. These bacteria play a key role in keeping children mentally and physically healthy and also reduce the risk of illness and disease.
Symptoms of a poorly functioning gut include uncomfortable digestion, stomach aches, poor nutrient absorption, poor immunity and sleep, mood fluctuations and general fatigue. All can have a detrimental impact on children. The gut microbiome is established in the early years of life. It’s particularly important to support a child’s gut microbiome to thrive while they’re growing. In fact, it is believed that before the age of four or five children’s microbiome remains flexible. This is a great time to build a strong and healthy gut health in children. Beyond this age the microbiome is harder to change as it becomes well established. Everyone’s microbiome is unique and, interestingly, diet can be responsible for up to 75% of this variation!
Elimination of Waste
The gut removes waste from the body. This is important to help support liver function. So, to keep a child’s bowel movements regular (and prevent uncomfortable constipation), encourage a diet with plenty of fibre. For instance, include wholegrains, veggies and fruit in their diet. This will keep the bowels regular and also feed the healthy gut bacteria. Water is also important to help keep bowel movements soft and regular.
The Immune System
The gut is home to 70% of the body’s immune system. It is also the main entry point for bugs to get into the body. Therefore, if a child’s gut is not a strong barrier they will be more likely to pick up nasty bugs. This can lead to illness. Research suggests that a poor balance of bacteria in the gut during early childhood can increase risk of gut-related allergies like asthma and eczema. Advise parents that they can help build their child’s immunity by

fuelling the good bacteria in their gut. This will, in turn, keep children feeling energetic and healthy.
The Gut-Brain Axis
The Gut-Brain Axis is the physical and chemical connection between the gut and brain. To clarify, it is a network of millions of nerves sending messages both ways. Chemicals called neurotransmitters, such as serotonin and GABA (which controls feelings of fear and anxiety), are sent to and from the brain. Many of these are produced in the gut. A thriving, healthy gut microbiome contributes to production of chemicals and signalling messages for good mental and physical health in children.
The Role of Probiotics
Probiotics are the “healthy” bacteria that make up the gut microbiome. Probiotics work to maintain health and immunity. They also fight inflammation and disease. Parents can boost the good bacteria in a child’s gut by feeding them probiotic rich foods. Good bacteria can help to form a strong, healthy microbiome. A probiotic supplement is also an option.
Researchers are still learning about all the benefits of probiotics and how they work. Probiotics may help with digestion, preventing
infectious diseases and even playing a role in maintaining a healthy weight.
Some studies say probiotics help children with digestive issues such as:
• Constipation
• Inflammatory bowel disease
• Irritable bowel syndrome
• Infectious diarrhea
Though it is unclear if probiotics benefit children, it’s clear they typically won’t cause harm in healthy children. However, pharmacy teams should recommend parents wait until a child is over 1 year of age before giving probiotics.
Children who are seriously ill or who have a compromised immune system should consult their GP before taking probiotics. Some studies suggest that children with a central line or port should also avoid probiotics. In children with these medical devices, there have been reported cases of sepsis.
Fibre
A child’s diet should contain fibre as an essential component. It is required to achieve good gut health in children and different fibres help the gut in their own unique ways.
While we often think of fibre as a singular nutrient there are actually many different types, for example:
• Insoluble fibre: Wholegrain breads and cereals and the skin of fruit and vegetables help to soften bowel content, promoting regular (and comfortable) bowel movements.
• Resistant starch: This is a type of fibre which is not digested as normal by the body. Resistant starch is found in wholegrain cereals, legumes and starchy vegetables like potato. It travels to the large intestine where it feeds good bacteria in the gut. These good bacteria produce what you need for a healthy digestive system and protection against disease.
• Prebiotics: These are another type of fibre which also feed the friendly bacteria in the gut. This provides another nourishing food source to the healthy bacteria in your gut. The great news is prebiotics are found in foods that are very child-friendly and delicious. Think bananas, apples and oats plus foods that are easy to sneak into meals like barley, onion or flaxseed.
• Soluble fibre: These help to slow the emptying process in the stomach, which can help children to feel fuller for longer. Soluble fibre is found in fruits, vegetables, oats, barley and legumes.
PHARMACYNEWSIRELAND.COM | 25
Baby Focus: Baby News
In4Kids – First Clinical Trial Network in Ireland
A new network putting children at the centre of decision-making in healthcare was launched today at University College Cork.
Lead for the In4kids network and INFANT Centre Director, UCC, Professor Geraldine Boylan
psychological differences from adults. Medicines and treatments made for adults therefore cannot simply be applied to children.
Professor Geraldine Boylan, lead for the In4kids network and INFANT Centre Director, UCC, said: “All children must have access to innovative therapies and medicines that have been developed with the same rigour and urgency as those developed for adults. We have a great team of investigators in our network and in4kids will support them to roll out the latest clinical trials for children across Ireland.”
Funded by the Health Research Board (HRB), In4Kids, the Irish Network for Children’s Clinical Trials, will support innovative clinical research and trial design for children in Ireland. It is the first clinical trials network in Ireland to focus on children’s health.
Better patient outcomes
Evidence shows that researchactive hospitals have better patient care outcomes. In4kids will allow healthcare staff and researchers throughout Ireland to work together through a multidisciplinary network, with access and support for participation in national and
international clinical trials with particular emphasis on rare paediatric diseases and high medical need areas.
The network is developing educational and training resources for everyone involved in clinical trials and will soon establish a young persons’ advisory group. The network also aims to ensure that children and their families are involved in clinical research from an early stage and that the research is relevant and accessible to them.
In4kids is the Irish hub in the c4c network, a pioneering European

network that aims to facilitate the development of new drugs and other therapies for the entire paediatric population.
Children are not little adults
Paediatric patients have developmental, physiological and
Professor Helen Whelton, Head of College of Medicine and Health, UCC said, “In4kids is working to ensure Ireland produces excellent clinical research and clinical trials to benefit all children. We are launching a paediatric network to ensure that every child is seen and heard and has access to the best possible therapies and interventions. Our children deserve and must have the same access to high quality, evidence-based health care as adults.”
As part of the launch, leading experts addressed the challenges and opportunities for clinical trials in children in Ireland as well as announcing a new collaboration between the Glucksman and In4Kids.
10th condition for National Newborn Bloodspot Screening Programme
The Minister for Health Stephen Donnelly has approved a recommendation from the National Screening Advisory Committee (NSAC) to add a group of conditions known as Severe Combined Immunodeficiency (SCID) to the National Newborn Bloodspot Screening (NBS) Programme. When implemented, this will bring to 10 the number of conditions screened as part of what is commonly known as the ‘heel prick’ test in Ireland. Minister Donnelly said, “Expansion of newborn screening has been a priority for me as Minister, and I am pleased to approve the recommendation from the National Screening Advisory Committee for addition of the group of SCID conditions to the National Newborn Bloodspot Programme. I want to commend the NSAC and HIQA (Health Information and Quality Authority) for the extensive work and thorough process undertaken in assessing the evidence for the expansion of this programme. I have asked the HSE to begin planning for the implementation of this recommendation on SCID, which will
bring the number of conditions we screen for in Ireland to
10.”
The NSAC considered a comprehensive Health Technology Assessment (HTA) report from HIQA on the evidence for the addition of SCID to the NBS programme at its meeting in December 2022, and made its recommendation based on the evidence and advice in the HTA. SCID is a group of rare but serious inherited conditions which are almost uniformly fatal in the first year of life without appropriate treatment. National and international evidence consistently suggests that earlier identification and earlier treatment for SCID results in better clinical outcomes for the child. The estimated prevalence of diagnosed SCID in Ireland is relatively high at 1 in 39,760 births, with 27 patients diagnosed from 2005 to 2020. The ongoing expansion of the NBS programme is a priority for the Minister and the NSAC, and several other rare newborn conditions are undergoing consideration. At its December 2022 meeting, the NSAC decided to ask HIQA to carry out a HTA for the addition of Spinal Muscular Atrophy (SMA). It is expected that HIQA will commence this work early in 2023.
PHARMACYNEWSIRELAND.COM
All children must have access to innovative therapies and medicines that have been developed with the same rigour and urgency as those developed for adults
Call for papers: make your contribution to Irish Pharmacy News






Articles



Research Papers
Reviews
Programme Descriptions
Reports
Case Reports

Letters to editor
In-depth review articles critique fundamental concepts, issues, and problems that define a field of research or practice and support advanced practitioners as well as aspiring early-year pharmacists.
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients with the aim to improving pharmacy practice.
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions.

Contact: Kelly Jo Eastwood at: kelly-jo@ipn.ie or Aoife Jackson at: aoife@ipn.ie

PHARMACYNEWSIRELAND.COM
Baby Focus: Breastfeeding
The Benefits of Breastfeeding
Katie Mugan is the founder of Nursing Mama, a nurse by profession –a registered General, Pediatric & Public Health Nurse and an International Board Certified Lactation Consultant. Katie runs a busy private practice educating & supporting parents and health care professionals regarding breastfeeding. Katie is going to share her knowledge on supporting breastfeeding parents in the community setting
main finding is lack of support and conflicting advice from health care professionals.
It is no surprise to anyone in the medical profession to hear that Ireland has one of the lowest breastfeeding rates with only 62.3% initiating breastfeeding after birth. This is significantly lower when compared with Australia 90%, UK 81% and in the USA 79%. Our rates further drop to only 31.2% of mothers breastfeeding at 3 months.
There is no dispute that breastmilk is the optimum form of nutrition for an infant. However, it is every parents choice on how they choose to feed their baby and they should be supported also. If breastfeeding is initiated, every woman will produce breast milk specific to the needs of their baby. It provides everything a baby requires for healthy brain, growth and development and changes continuously to meet these needs. Breastfeeding is not only a source of nutrition but has amazing health benefits to both mother & baby. Breastfeeding is shown to reduce the risk of common infant illnesses -otitis media, respiratory tract infections and gastrointestinal infections and SIDS along with long term benefits such as childhood obesity and diabetes. For mothers, it reduces the risk of Ovarian and breast cancer, diabetes and cardiovascular disease. The benefits of breastfeeding are undeniable so why are our rates so low? Although multi factorial, one
Often the first port of call for any new parent for advice is their local pharmacy. Meeting a friendly, supportive face when in the midst of life with a newborn can have a huge impact on a parents experience. Community pharmacists are the most accessible healthcare provider meeting breastfeeding mothers regularly. They can have a direct impact on this patient demographic, providing support and education whilst alleviating concerns regarding medications and breastfeeding. Taking medications while breastfeeding can often lead to breastfeeding being interrupted when not necessary.
These brief interruptions can have a significant impact on a breastfeeding journey and this should not be the first recommendation unless absolutely certain this medication is not suitable for a lactating woman. There are several resources available to help pharmacists regarding medications and the lactating mother and the use of same. The Academy of Pediatrics regards LACTMED as the most reliable and up to date resource for medication use in lactating women. Another resource used widely is ‘Medications & mothers milk’ and a fantastic resource to share with parents is ‘The breastfeeding network.org.uk’. This offers a huge amount of information regarding illnesses, procedures, medications in breastfeeding mothers. Providing this resource allows parents make informed decisions in combination with their health care provider regarding their own situation.
Many parents will seek advice for over-the-counter medications so being familiar with commonly used products is beneficial.
Analgesics are one of the most commonly requested OTC medications. Ibuprofen is considered safe but best to avoid any combinations containing codeine. Come the good weather/ hay fever season you will have an influx of mothers looking for OTC remedies. Non-sedating medications are preferential here and considered safe for short term use. During the winter season, the demand for cold & flu remedies are highest. Many of these products contain pseudoephedrine which can lead to a dip in milk supply and so are best avoided for lactating mothers. During challenging times, the pharmacist can play a pivotal role in supporting a breastfeeding mother. Simple products and advice can stop a mother giving up breastfeeding altogether. Offering simple and basic tips on nipple care can be so beneficial to a lactating mother. Nipple discomfort is normal in the early days but constant, significant pain is not. This demonstrates an issue and if not rectified quickly may lead to nipple trauma or cessation of breastfeeding. No nipple preparation is required before baby arrives. Ensuring a good latch and attachment is priority from the offset. Nipple creams and balms can provide comfort. Mutimam compress, can feel lovely to a mom with tender nipples when applied from the fridge between feeds. Lanolin was once the balm of choice, however, more research is indicating that it can lead to higher rates of infections when used on cracked nipples. There is also a risk of allergic reactions making sore nipples worse and so many lactations consultants are steering clear. Good wound care is necessary when dealing with cracked nipples. Silver cups are becoming more popular for nipple care. Silver is a natural antimicrobial, antifungal, antibacterial metal and
has anti inflammatory properties. However, like any product if not used correctly can lead to further wound breakdown. A moist wound environment is needed for wound healing but too moist leads to wound breakdown so ensure clients don’t leave them on too long between feeds.
Simple OTC products which can help- nipple shields, nipple evertors, breast pads, breast pumps (consider stocking Hospital grade pumps for rent). Nipple shields get a lot of bad press but they can help a mother while waiting on help. Always look for the root cause as to why they are needed is of utmost importance. Nipple evertor- I love them!!
Basically, they suck out and make a nipple more pronounced. If a mother is concerned re flat or inverted nipples, these are great to pop in a hospital bag just incase. Many mothers may need to use a pump, not by choice in the early days but out of necessity. Hospital grade pumps are recommended in this situation and parents will generally rent them.
However, if you consider stocking these pumps, it allows parents to collect directly from you reducing the wait time for parents on home delivery. Having a good breastfeeding section within your pharmacy leads parents to shopping local for all breastfeeding needs rather than online. This also increases the feeling of a supportive breastfeeding pharmacy. As medication experts dealing with the public daily, Pharmacists are in the best position to offer advice regarding breastfeeding and medication use. Having a clear understanding of some simple products that can assist breastfeeding mothers during challenging times can lead to better outcomes and help improve our national breastfeeding rates.
https://nursingmama.ie/

28 | PHARMACYNEWSIRELAND.COM
Written by Katie Mugan, Nursing Mama

















MAM Easy Start Self-Sterilising Bottle. Look! The bottle that babies love! Parents are demanding and we at MAM are too. That’s why we develop products that are unique in design and function, like the MAM Easy Start bottle. 94% of babies accept the MAM Skin Soft™ teat1 and the bottle has a self-sterilising feature and vented base which helps to reduce colic, so parents can feel confident and babies feel good. 1 Market research 2010-2020, tested with 1,572 babies. 2Field study, Austria 2011, tested with 73 mothers of colicky babies / Market research, USA 2010, tested with 35 mothers of colicky babies. Teat Self-sterilising in 3 easy steps: 1. Fill with 20ml of water 2. Put the bottle parts together 3. Heat in the microwave for 3 minutes Order Now from your Eurosales International Sales Representative or telephone now on 01 405 0900 / 01 450 7771
Baby Focus: Dental
Dental Hygiene in Infants and Children
How can pharmacists encourage good dental hygiene among infants and children?
Children are losing crucial days of their education each year due to rotting teeth, as well as suffering pain, sleepless nights and missing out on doing the things they enjoy the most - which is being a child! Not to mention time taken off work by parents and carers.
Children begin to lose their teeth around aged 6-7, with the last being lost around age 12-13. This is too long for a child to be subject to pain and discomfort. Often, it is not possible to restore decayed teeth in children, and extractions are required under general anaesthetic.

as recommended by the OHF. The key aim is to promote and protect people’s oral health by improving their diet and oral hygiene and encouraging them to visit the dentist regularly.
Key points for keeping deciduous teeth cavity-free:
• Brush twice daily with a fluoride toothpaste
• Limit sugar
• Visit the dentist regularly
Risk Factors for Tooth Decay
Encouraging Good Dental Hygiene
As a mother of two children aged 5 and 7, I understand and appreciate the need for more health professionals to understand more about Dental hygiene; it’s important as a Dentist and as a parent.

Tooth decay, an almost entirely preventable disease, remains the single most common chronic disease of childhood and the number one reason for childhood hospital admissions. The Oral Health Foundation (OHF) prioritises improving oral health for all, to ensure young people are given the very best start in life by providing them with the means to have a healthy mouth.
Tooth decay is largely the result of not brushing teeth twice a day with a fluoride toothpaste and consuming too much sugar. Many people believe baby (deciduous) teeth do not matter because they will be replaced by the adult teeth, however deciduous teeth play a crucial role in a child’s emotional and physical wellbeing. Children need healthy teeth to eat nutritious foods, speak clearly and smile brightly. Deciduous teeth are essential for the proper development of adult teeth, acting as a spacer, guiding the permanent teeth into position. If lost prematurely, results in crowding and malocclusion.
Acting to prevent tooth decay doesn’t have to be complicated or difficult, it can be structured around educating caregivers so we can create good habits from the outset. Prevention is better than cure; and pharmacists are in a unique position to provide oral health advice, a cost-effective intervention that can save money in the long-term and reduce the number of children needing time off school because of tooth decay.
Call to Action
Achieving good dental health for all children requires a whole system approach. At the frontline of healthcare, pharmacists have a substantial role in influencing behaviour to improve the oral health of children. Pharmacists are positioned to give accessible professional oral health advice, in a friendly, comfortable atmosphere
Tooth decay is a result of the destruction of the hard tissues of the tooth by acids produced in the mouth when bacteria in dental plaque metabolises dietary sugars. Repeated and prolonged acid attacks will eventually cause the tooth surface to weaken and a cavity to form which may lead to pain and infection. The risk of tooth decay increases in more deprived areas where the imbalance in income, education, employment, and neighbourhood circumstances affect the life chances of children’s development.
Studies show children are more at risk of developing tooth decay if they are
• Eating a poor diet
• Brushing their teeth less than twice a day with a fluoride toothpaste
• From deprived backgrounds
Pharmacists have the opportunity to engage with members of the community who are caregivers of babies and young children to advise on good dental health. With an aim to improve the oral health of all children and reduce the oral health gap for disadvantaged children. Pharmacists are a good source of information to advise on caring for oral health, and to recommend the most effective products for individual needs. Recommending a range of oral health products such as toothbrushes and fluoride toothpastes.
Tooth Brushing
Daily application of toothpaste to teeth reduces the incidence and severity of tooth decay in children. To maximise prevention of tooth decay, children should brush their teeth at least twice a day with a fluoride toothpaste. Children in more deprived areas are less likely to brush their teeth at least twice a day.
Caregivers of babies should be encouraged to clean twice daily from the day the first tooth appears, using a soft baby brush, with a smear of fluoride toothpaste. All children should brush twice a day with a fluoride toothpaste, last thing at night and at one other time of day.
Adult toothpaste is perfect for the whole family, children under
30 | PHARMACYNEWSIRELAND.COM
Written by Dr Madelaine Jackson, Dentist of the Year 2022, Cosmetic Dentist of the Year 2022, Best Aesthetic Dentist 2021 Instagram @DoctorMadelaine
step by step
toothpaste indicator


Jordan Step by Step
Ergonomic handle


Children have different needs as they grow older. Step by Step is a unique kids range that follows the children's development and offers tailored design with different features to make brushing easy and effective at every age. The handle, head size, bristles and design are all tailor made to help you establish good dental care habits from the first tooth. Choose the one that fits your child.



ring
Order Now from Your Sales Representative or Phone 01 405 0900 / 01 450 7771
Baby Focus: Dental
3 years old should use a smear and 3-6-year-olds a pea sized amount; Kids toothpastes are great but adult toothpastes are better; my kids love being minty fresh. There is no need to rinse after brushing, the first few occasions may feel intense for the kids but it is only reducing the fluoride. Avoid eating and drinking for at least one hour after brushing.
Electric toothbrushes can be introduced from age 3.

Toothbrushing should be supervised by an adult until at least age 7.
Dietary Advice
The pharmacist has a vital role to support the education being given in the dental practice by reinforcing healthy eating messages, with a reduction in and frequency of sugar consumption.
For babies:
• Bottle fed babies should be introduced to a free-flow cup from 6 months and bottle discouraged from 12 months. Do not give the baby a bottle overnight, the milk bathes the teeth causing tooth decay
• Milk and water are the only healthy drinks
• Only milk or water should be given in bottles
• Avoid adding sugar to foods or drinks
For all children:
Give healthier eating advice routinely to promote good oral and general health. Eat a nutritious diet and limit snacking. The main message is to reduce the number of sugary foods and drinks
• Reduce the quantity and frequency of foods and drinks that contain sugar
• Juice has no real place in a child’s daily diet
• Administer sugar-free medicines where possible
Practical advice on how to limit sugar intake with food and drink:
• Water and milk are the only safe drinks
• Looking out for ‘hidden’ sugar in foods and drink
• Eat whole foods
• Breakfast cereals are notoriously high in sugar, double check the labels to what extent
• Avoid adding sugar or jam to foods, most foods already have sugar in them so more is not needed
• Deserts and treats only on special occasions, everyone likes a treat, just in moderation!
Food Myths
• ‘No added sugar’ is not the same as ‘sugar-free’
• Sugar-free often contain sweeteners, that can also cause tooth decay
• Many health foods snacks such as cereal bars and dried fruits have deceptively high sugar levels
• Fruit juices and smoothies are high in ‘free’ sugars
Dental Attendance
A significant proportion of the population are not currently registered with a dentist, which makes the pharmacy an important source of accessible oral care advice.
Children should see a dentist by their first birthday, to familiarise with the dental setting and for professional oral health advice. Getting children used to the environment from an early age will prevent fear in the future. Keeping primary teeth cavity-free also ease
the fear and discomfort children might feel if the dentist needs to treat or remove a decayed tooth.
A dentist can be a fun and exciting place for kids, tell them about the adventure they will go on, excite them about the machines and dental chair, and more importantly there us a strong chance they will leave with a sticker to show off to their friends!
Oral Health in the Community
I am passionate about oral health and have been involved in a local health initiative to deliver oral health education to school and nurseries. Last year I visited a local pre-school and provided oral health education for 3-4 years. We did a fun-based lesson on the importance of keeping teeth clean, going to the dentist and limiting sugar. I brought with me a puppet, ‘Doug the Dentist’ to demonstrate tooth brushing technique and different types of manual and electric toothbrushes.
I gave all the kids a free pack to take home which included:
• Toothbrush
• Toothpaste
• Toothbrushing chart
• Stickers
I’m proud of the education I provided and hope to make further visits to this year.
The key is creating health habits at home that will improve long term dental health.
Tooth decay can have a serious impact on children’s physical and emotional health, and extractions at such a young age can signal a lifetime of poor oral health ahead. We need to work together to protect our children from this devasting but preventable disease. Pharmacists are uniquely positioned to offer oral health advice for parents and caregivers of young children to promote good oral health to children in the community.
National Smile Month
National Smile Month is a charity campaign usually in June. The OHF will be raising awareness of important oral health issues and preventing oral health inequalities by sharing important oral health messages. Look out for Marketing material that may be available as new facts we can share with parents and kids.
Making
Every Contact Count
(MECC), How NICE resources can support local priorities
MECC is an evidence-based approach to improving people’s health and wellbeing by helping them change their behaviour. MECC uses brief and very brief interventions, delivered whenever the opportunity arises in routine appointments and contacts. The person is encouraged to think about a change and offered help such as a referral or further information. A brief intervention involves a conversation with encouragement. Supporting people to take action to improve their lifestyle is central to MECC.
SMILE4LIFE is a programme of initiates to improve dental access and oral health in England. Reduce health inequalities and improve oral health in children.
Diet is highly important for the health of your mouth. A pharmacist should also be able to give you advice about how foods and drinks can affect your teeth. Large amount and frequent consumption of sugary foods and drinks is the biggest cause of tooth decay. Cutting down on sugary foods and drinks is one of the OHD’s key messages.
32 | PHARMACYNEWSIRELAND.COM
With CleanMaximiser technology, green bristles turn yellow when it’s time to change
































































USED www.prl ie pgsales@prl ie +353 1 257 4650 PRL SALES ULC, Greenogue Business Park Rathcoole Co. Dublin
your brush head
NEW
Dentists recommend to change
every 3 months
Baby Focus: Supplements
Recommending Supplements for Infants and Young Children
Written by Dr Annemarie Bennett, Registered Dietitian and Assistant Professor in Dietetics, Trinity College

important during periods of rapid bone development, such as infancy and early childhood. Research has also highlighted the potential role of vitamin D in long-term health outcomes, such as reducing the risk of heart disease, diabetes, and the Metabolic Syndrome, making the prevention of deficiency a public health priority.
Vitamin A
Vitamin A is particularly important for the development and maintenance of eyesight and plays a role in growth and the development of healthy body tissues. Vitamin A deficiency is rare in high-income countries, but when it does occur, it can result in night blindness and xeropthalmia (dryness of the conjunctiva and cornea of the eye).
The main dietary sources of vitamin A are of animal origin, and include milk, cheese, eggs, fortified spreads, yoghurt, meat, and meat products. Non-animal sources of vitamin A include vegetables such as carrots and sweet potato. Through an appropriately varied diet alone, infants and young children should achieve recommended intakes of vitamin A. Supplementation with vitamin A among infants and young children is not recommended unless advised by a medical doctor.
Vitamin B
There are several different kinds of B vitamins, and they have many different and important functions in the body, to include facilitating the release of energy from food, protecting the nervous system, and maintaining healthy blood cells. Deficiencies in B vitamins are rare among children in high-income countries. A key
reason for this is that B vitamins are found in a wide range of foods, to include vegetables, milk, cheese, meat, fish, poultry, eggs, and fortified cereals. Vitamin B requirements should be met through an appropriately varied diet alone, with supplementation only advised when recommended by a medical doctor.
Vitamin C
Vitamin C is important for maintaining the health of skin, gums, blood vessels, bones, and cartilage, and for supporting immunity and healing. Poor vitamin C intakes over several months can lead to an inflammation of the gums – a condition called scurvy, which is easily treatable with the reintroduction of vitamin C. However, vitamin C is found in a wide variety of fresh fruits and vegetables, and especially in citrus fruits, such as oranges and limes, making deficiency uncommon. Excessive vitamin C intakes can lead to stomach pains and diarrhoea, and as such, vitamin C supplements among infants and young children are not recommended unless specifically advised by a medical doctor.
Vitamin D
Vitamin D helps our body to absorb calcium and is therefore essential for musculoskeletal and dental health. It is especially
Vitamin D is made in our skin when it is exposed to UV light from the sun’s rays. However, prolonged direct exposure to sunlight is not recommended for any person, and especially infants and young children, given the impact this has on shortand long- term skin cancer risk. Vitamin D can be consumed in food, but natural food sources of vitamin D that are suitable for infants (once weaning commences around 6 months of age) and young children are relatively few, e.g., oily fish and eggs. Foods fortified with vitamin D have become more commonplace and are important contributors to dietary intakes of vitamin D, e.g., cereals, yogurts, cheese, cow milk, and infant and growing up milks. Fortified infant milks have become notable sources of vitamin D for infants over the past decade, and even more so in recent years, as EU legislation was amended to permit higher amounts of vitamin D per 100kcal milk formula. These advances in food sources of vitamin D increase the likelihood of meeting vitamin D recommendations, especially among infants consuming milk formula and young children consuming fortified milk.
For infants that are exclusively breastfed or are consuming relatively small amounts of milk formula, however, it is unlikely that recommendations for vitamin D will be met. To help overcome this, the HSE recommends a daily supplement of 5 micrograms (mcg) vitamin D from birth to 12 months of age for infants that are:
• Breastfed; and/or,
• Taking less than 300mls (10 ounces) infant formula per day.
For all young children aged 1-4 years, the HSE recommends giving a supplement of 5 mcg
vitamin D everyday throughout winter, typically from Halloween to St Patrick’s Day. This recommendation was made because skin cannot synthesise vitamin D during the winter months in Ireland, when sunlight is weaker and limited. With sunlight contributing little or nothing to vitamin D stores during this time, it is difficult to meet vitamin D recommendations through diet alone and a vitamin D supplement is needed. However, from midMarch to October, dietary sources of vitamin D with responsible exposure to sunlight typically ensure requirements are met. When supplements are recommended, liquid supplements containing only vitamin D are advised for infants and young children. Chewable or tablet-type supplements pose a choking risk and should be avoided.
Iron
Iron is essential for growth and the development of healthy blood cells. Infants are born with a 6-month store of iron that they accumulate from their mother over the course of pregnancy. From about 6 months of age, these stores have run low, and infants and young children need to consume sufficient iron from their diet.
Food rich in iron and suitable for children aged 6 months and upwards includes beef, lamb, and pork. Other foods that contain iron include eggs, fortified cereals, and leafy greens, although iron from these foods is less easily absorbed. Vitamin C increases the amount of iron absorbed from food, so consuming fresh fruits and vegetables with iron-containing foods will optimise absorption. Insufficient iron in the diet can lead to iron-deficiency anaemia, which is characterised by tiredness, pallor, poor appetite, and difficulty fighting infection. If there are concerns about iron deficiency, it is important to recommend a visit to the GP, who will investigate accordingly. Given the risks of iron overload, iron supplementation is only advised for infants and young children when specifically recommended by a medical doctor.
34 | PHARMACYNEWSIRELAND.COM
LET
LET US HELP YOU MANAGE DIABETES
Identified as preferred blood glucose test strips with associated meters by the MMP.
Identified as preferred blood glucose test strips with associated meters by the MMP.
SMART
SMART
SYSTEM ACCURACY
SYSTEM ACCURACY
of 4SURE SMART DUO test results are within ± 0.83 mmol/L (low glucose levels) or ± 15% (high glucose levels) of laboratory reference method test results. 4

99.33% of 4SURE SMART DUO test results are within ± 0.83 mmol/L (low glucose levels) or ± 15% (high glucose levels) of laboratory reference method test results. 4

SMART DUO
SMART DUO
Blood Glucose monitoring System (IDEAL FOR TYPE 1 & 2 PATIENTS). Blood

TO ORDER YOUR FREE METER CONTACT: 1800 26 26 26
TO ORDER YOUR FREE METER CONTACT: 1800 26 26 26
Clonmel Healthcare Ltd., Clonmel, Co. Tipperary. Always read the instructions before use. 2021/ADV/4SU/012H. Date prepared February 2021. 1. Haematocrit range 0-70% (blood glucose), 10-70% (ϐ-ketone). 2. For driving with diabetes, follow DVLA guidelines. 3. Follow NICE guidelines “Diabetes in pregnancy: management from preconception to the postnatal period” 4. Assessment of System Accuracy, Intermediate Measurement Precision, and Measurement Repeatability of a Blood Glucose Monitoring System Based on ISO 15197. Jendrike N, et al., J Diabetes Sci Technol. 2018 Dec 14. Suitable for Gestational Suitable for gestational patients3 Ketone β
blood glucose and ϐ-ketone test strips Meal Pre AC Post PC 0-70% HCT
for drivers Pre and post meal markers
for drivers2 Wide haematocrit range1 Bluetooth connectivity
Affordable
Suitable
Suitable
Additional Feature Additional Feature
Glucose & ß-Ketone monitoring System (IDEAL FOR TYPE 1 PATIENTS).
DIABETES CARE
Clonmel Healthcare Ltd., Clonmel, Co. Tipperary. Always read the instructions before use. 2021/ADV/4SU/012H. Date prepared February 2021. 1. Haematocrit range 0-70% (blood glucose), 10-70% (ϐ-ketone). 2. For driving with diabetes, follow DVLA guidelines. 3. Follow NICE guidelines “Diabetes in pregnancy: management from preconception to the postnatal period” 4. Assessment of System Accuracy, Intermediate Measurement Precision, and Measurement Repeatability of a Blood Glucose Monitoring System Based on ISO 15197. Jendrike N, et al., J Diabetes Sci Technol. 2018 Dec 14. Suitable for Gestational Suitable for gestational patients3 Ketone β Affordable blood glucose and ϐ-ketone test strips Meal Pre AC Post PC 0-70% HCT Suitable for drivers Pre and post meal markers Suitable for drivers2 Wide haematocrit range1 Bluetooth connectivity
US HELP YOU MANAGE DIABETES
System
Blood Glucose & ß-Ketone
Additional Feature Additional Feature
Blood Glucose monitoring
(IDEAL FOR TYPE 1 & 2 PATIENTS).
monitoring System (IDEAL FOR TYPE 1 PATIENTS).
99.33%
DIABETES CARE
Baby Focus Management of diabetes in pregnancy: before, during and after pregnancy
Written by: Christine Newman1, 2 - Fidelma Dunne2, 3
1Department of Diabetes and Endocrinology, Addenbrooke’s Hospital, Cambridge University Hospitals
2Diabetes Collaborative- Clinical Trials Network, University of Galway
3Centre of Diabetes, Endocrinology and Metabolism, Galway University Hospital
Diabetes in pregnancy will affect 16% of women during their pregnancy. The vast majority of these cases are gestational diabetes mellitus (GDM), however nearly 1% of pregnant women in Ireland will enter pregnancy with type 1 or type 2 diabetes mellitus (collectively termed pregestational diabetes mellitus or PGDM).
During pregnancy
The diagnosis of GDM can be extremely stressful for some women and the risk of anxiety and depression can increase at this time, particularly in women with a history of low mood/depression. Around the time of diagnosis women will receive education regarding dietary and lifestyle changes which can help reduce blood glucose levels and they will also be shown how to test their blood glucose levels. Issues which tend to arise around this time are
Avoiding excess gestational weight gain (GWG)- there are safe limits for weight gain in pregnancy. Adhering to these limits can help reduce the risk of blood pressure problems and having a baby that is large for gestational age.
Post-partum
While obstetric outcomes have improved over the last three decades, many women with diabetes in pregnancy will face complications like hypertension, premature birth, Caesarean section, macrosomia (birth weight >4kg) and further more severe complications like stillbirth and congenital anomaly are rare, but still occur.
Adequate preparation and excellent glucose control during pregnancy can help to reduce many of these complications.
Gestational diabetes (GDM)
Pre-conception
GDM occurs most frequently in women who are older, overweight or obese, have a history of previous GDM or polycystic ovarian syndrome, have previously had a child who was large at birth or with a congenital anomaly, have a family history of diabetes or are from Africa, south east Asia or south America. Most obstetric centres will test for diabetes at a booking visit using a combination of haemoglobin A1c (HbA1c) and
fasting glucose. Women who have normal readings, but still have risk factors will be tested again at 2428 weeks of pregnancy.
For women with risk factors for GDM it is important that they pay particular attention to modifiable risk factors. This includes:
The use of folic acid which is recommended for all women is especially important in this cohort, and many societies advise using higher doses of 5mg folic acid in women who are overweight or obese


Cessation of any medications which could potentially be harmful. A review of medications may identify medications like statins or ACE inhibitor which can potentially be harmful. If these medications are necessary, alternatives should be sought
Optimising weight and body mass index prior to pregnancy
Other general advice should include smoking cessation, vaccine uptake (particularly rubella, influenza and Covid-19)
Frustration with checking blood glucose levels 7 times per day. Additionally, blood glucose test strips have not traditionally been reimbursed for women not on a General Medical Scheme (GMS), and the cost implications of a GDM diagnosis can be very difficult for some patients. Guidance from a pharmacist about the most cost efficient strips is extremely useful.
During pregnancy the targets for good glucose control are a fasting blood glucose of <5.3 mmol/L and a glucose of <7.8 mmol/L two hours after food.
Even with dietary and lifestyle measures, up to 40% of women will need some form of pharmacological therapy to optimise their blood glucose. Options include metformin, which is not currently approved under the HSE protocol for management of GDM, but which is used off-licence; and insulin. Insulin can be given multiple times per day and some women will require a long acting basal insulin and up to 3 injections of short-acting insulin before food. Additional support, reassurance and counselling regarding safety is really important at this time.
After pregnancy, women with a history of GDM can stop testing their blood glucose levels. All women should be offered follow up testing 3-6 months after delivery to ensure that they no longer have high blood sugars. This is usually done at the delivery hospital however if this can’t be facilitated for practical reasons, transport etc it is essential that some form of glucose testing be done in the postpartum period. Reminding and encouraging women to attend these appointment is critical as it’s a great opportunity to address weight reduction, diet, lifestyle and measures to reduce the risk of future GDM or type 2 diabetes. Breastfeeding, which has also been shown to reduce the risk of type 2 diabetes in the future, should be encouraged.
Pregestational Diabetes
Women who enter pregnancy with type 1 or type 2 diabetes face higher rates of, and more severe complications that women with GDM. Good glycaemic control is essential to prevent devastating complications like congenital anomaly and perinatal death.
Pre-conception
Many of the factors listed above are equally relevant in women with PGDM including high dose folic acid use, smoking cessation, stopping harmful medications and vaccination
The need to optimise body weight remains extremely
36 | PHARMACYNEWSIRELAND.COM
Christine Newman
Professor Fidelma Dunne
important in this group as an increasing number of women with PGDM are entering pregnancy with BMIs in the overweight range
A review of diabetes medications is particularly important in this group
o For women with type 2 diabetes, agents like sodium glucose transport 2 inhibitors, glucagon like peptide 1 agonists and DDP4 inhibitors have not been sufficiently studied in pregnancy and there is some evidence to say they may be harmful. These agents should be stopped in advanced of trying to conceive.
o Women with type 1 diabetes who are trying to conceive are entitled to continuous glucose monitoring (CGM). CGM has been shown to reduce neonatal intensive care admission and large for gestational age births. It does this by helping the woman achieve very good glucose control pre-pregnancy.
All women with diabetes should aim to enter pregnancy with a HbA1c <6.5 mmol/mol.
All women with PGDM should have a review of the eyes and kidney function before becoming pregnant, as pregnancy can cause additional complications in this group.

During pregnancy
Women should continue on folic acid until the end of the first trimester
Women with type 2 diabetes should test their glucose levels 7 times per day in pregnancy, before and 2 hours after each meal
Women with type 1 diabetes who are not already using CGM should be started on it once pregnancy is confirmed. Women should aim to spend more than 70% of the day and night
with glucose readings between 3.5-7.8 mmol/L
For women with both type 1 and type 2 diabetes, pregnancy is a time of insulin resistance. Higher doses of insulin will likely be needed throughout pregnancy, and by the third trimester women often require twice the dose of insulin that they needed at the start of pregnancy
Women with type 2 diabetes who were on oral agents before pregnancy very often need insulin in pregnancy
Child and Adolescent Mental Health
Women should have eye screening during each trimester After pregnancy
Insulin requirements will usually return to the pre-pregnancy ranges
Particularly for women with type 1 diabetes, hypoglycaemia can be a concern – particularly around breastfeeding. They should be advised to eat prior to breastfeeding and may need to reduce their insulin dose.
The HSE received the interim report of the Inspector of Mental Health Services into the provision of Child and Adolescent Mental Health Services (CAMHS) in the State in early January.
Commenting, Damien McCallion, HSE Chief Operations Officer said, “This Mental Health Commission report comes at a time when we have a major CAMHS improvement process underway, and we will be putting a senior clinical/operational team in place to drive and support that process. This interim report, as well as the current prescribing review and other ongoing HSE audits in CAMHS, combined with the service improvement work underway, will all contribute to this process.
“The report makes systemic findings and conclusions, as well as highlighting concerns about the specific care provided to some
children. The HSE engaged with the Inspector of Mental Health Services in the course of her work and where specific concerns were identified, we immediately put in place targeted actions plans to address them. In the case of all children where concerns have been raised by the MHC in their report, these have been managed directly by the service caring for them.”
Commenting, Dr Siobhán Ní Bhríain, HSE National Clinical Director Integrated Care said, “The Child and Adolescent Mental Health Service is critically important to many young people and their families. We know that there are many challenges in the current service which can be continually
enhanced to better respond to young people in need, and we continue to work hard to improve the services we provide.
“A key recommendation of this interim report is that the HSE undertakes a review of cases within the CAMHS service that remain open - these are cases where a young person remains in the service but has not been seen for six months with a particular focus on physical health monitoring for those young people who have been prescribed neuroleptic medication.
“The HSE is putting the necessary plans in place to carry out this review so that we can be assured that children and young people
in our service are receiving appropriate and timely care reflective of their current and future needs.
“We are glad to note that the Mental Health Commission states in their report that many young people and their families have received excellent care and treatment within the oftenlimited resources of CAMHS teams who have nearly 20,000 cases nationally and see 225,000 appointments annually. While acknowledging the significant challenges we face, we encourage anyone engaged with a CAMHS service to stay connected to their team.”
PHARMACYNEWSIRELAND.COM | 37
News
Positive Step to Faster Medicines Access
The decision by Minister for Health, Stephen Donnelly T.D. to publish the Mazars Report has been welcomed by the Irish Pharmaceutical Healthcare Association as a positive step towards providing Irish patients with faster access to lifechanging new medicines.

for the HSE’s Corporate Pharmaceutical Unit, the HSE Drugs Group and the National CPE.
Child and Youth Mental Health Lead
especially important considering the many new advances in science and the potential to raise standards of patient care through faster access to newer and better medicines and treatments.
IPHA, which represents the major international biopharmaceutical companies in Ireland, commended the Minister’s decision to publish the report and to establish a Working Group to review and improve the reimbursement system for new medicines.
The organisation recognised that the initiative is the first of its kind since the passage of the Health (Pricing and Supply of Medical Goods) Act 2013, describing it as a valuable opportunity for key stakeholders, including industry and patient groups, to contribute to improved patient care and health outcomes.
IPHA said the Working Group’s role in reviewing and improving the reimbursement process was
It applauded the Minister’s decision to act immediately to enhance transparency in the reimbursement system through the introduction of a tracker system and indicative timelines, stating that it would result in better planning and management of applications for medicine reimbursement.
IPHA said it welcomed the opportunity to engage in the Working Group, to present its own reform proposals and to hear the view of other stakeholders. It stated, “We will put forward ideas in good faith and will also listen to what is asked of us. Our members are very conscious of industry’s responsibilities to improve the process in a collaborative way.
We will:
• Bring forward proposals to support the further development of national medicines policy.
• Present the case for an increase in personnel and IT resourcing
Pharmacy Role in Hygiene
• Explore ways for earlier reimbursement for certain treatments, such as early access schemes, as is done in other countries. IPHA companies are ready with some rare disease, cancer and end-of-life treatments that can be pathfinders for this new approach in 2023 and 2024.
• Advocate for an increase in the HSE’s decision authority table thresholds and more generally for a well-structured commercial framework, as exists in other countries.”
IPHA said there were “many other practical steps that can be taken to improve the processes that fully respect the HSE’s obligations under the 2013 Health Act. We will study the Mazars Report carefully and provide any observations arising from it to the Minister.”
Michael O’Connell, IPHA President said: “Over the past three budgets, the Government has allocated almost ¤100 million to new medicines. The announcement today is a further indication of the Minister’s continued commitment to ensure that patients have faster access to new, innovative medicines. I thank the Minister for driving this reform and bringing all stakeholders together in doing so”.
Advice on hygiene given by pharmacies has widened from oral care to infection control measures, according to a report by the FIP Global Pharmaceutical Observatory (GPO) published last month.
A literature review found educating people on hygiene measures such as handwashing and disinfection to be a novel community pharmacy service during the pandemic. The FIP GPO also conducted a cross-country survey through five FIP member organisations (n=60). More than half of the respondents reported that avoidance of respiratory, viral, communicable, and food and water borne infections were the most common “germ concerns” expressed to them by the public. The study also looked into current and future learning needs of pharmacy teams. The findings from the literature
review showed that the concept of providing hygiene care advice has been differently shaped preand post-COVID times. Before the COVID-19 pandemic, the area of focus was limited to oral hygiene. All studies reviewed in the literature reinforced the vital role of community pharmacists as the public’s first choice of healthcare provider in mitigating the spread of the disease as well as their prominent contribution to overall emergency management.
There was also an unequivocal need to support, train and educate community pharmacists and their teams to improve their knowledge
because the concept of increasing personal hygiene awareness is a focus area of community pharmacists in developed and developing countries.
The report states, “As evidenced throughout this report, community pharmacists and their teams can play a leading role in providing reliable recommendations and educating patients on health hygiene, engaging and empowering patients in self-care, and minimising the spread of contagious diseases, ultimately contributing to improving our communities’ overall health.”
Minister for Mental Health and Older People Mary Butler welcomed the opening of the recruitment process for the post of Child and Youth Mental Health Lead in the HSE. This key new role will provide leadership, operational oversight, and delegated management of all service delivery across child and youth mental health services across the country.
They will also be responsible for managing and coordinating service planning activities, partnership and capacity building, the development of service plans, and setting of service standards right across child and youth mental health services in Ireland.
The post holder will report to the HSE National Director for Community Operations and will be supported by a dedicated team for which funding has been provided.
This role, and the wider Child and Youth Mental Health office, will result in improved links with the National Clinical Advisor Group Lead Mental Health, which in turn will support the development of current and future youth mental health-related National Clinical Programmes.
Minister Butler stated, “The progression of this role has been a key priority for me over the past year, and it will play a crucial part in ensuring that integrated mental health services for young people have a more centralised and evidence-based focus within the HSE.
“We will see the completed reviews and audits arising from the Maskey Report, along with the Final Report of the Mental Health Commission on CAMHS later this year, which together will give us real time data never available before to support this new post. Importantly, there will be new support staff to underpin this welcome initiative. I will ensure that the HSE also progresses as quickly as possible the new post of National Clinical Lead for Youth Mental Health as announced in the Dáil over the last week.”
PHARMACYNEWSIRELAND.COM 38 News
IPHA President Michael O’Connell
LEADING
baby nutrition research
For over 100 years
SMA® Specialist Range
Did you know that feeding issues, such as colic, constipation, reflux & regurgitation occur in up to 55% of all infants in the first 6 months of life?1
management of reflux
Discover our full range at www.smahcp.ie/formula-milk
SMA LF® Lactose Free for babies with lactose intolerance management of colic and constipation

SMA High Energy® for medically identified high-energy needs
REFERENCES: 1. Iacono G. et al. Gastrointestinal symptoms in infancy: a population-based prospective study. Dig Liv Dis 2005;37(6):432–438.
IMPORTANT NOTICE: We believe that breastfeeding is the ideal nutritional start for babies and we fully support the World Health Organization’s recommendation of exclusive breastfeeding for the first six months of life followed by the introduction of adequate nutritious complementary foods along with continued breastfeeding up to two years of age. We also recognise that breastfeeding is not always an option for parents. We recommend that healthcare professionals inform parents about the advantages of breastfeeding. If parents consider not to breastfeed, healthcare professionals should inform parents that such a decision can be difficult to reverse and that the introduction of partial bottle-feeding will reduce the supply of breast milk. Parents should consider the social and financial implications of the use of infant formula. As babies grow at different rates, healthcare professionals should advise on the appropriate time for a baby to begin eating complementary foods. Infant formula and complementary foods should always be prepared, used and stored as instructed on the label in order to avoid risks to a baby’s health. The product be used only on the advice of independent persons having qualifications in medicine, nutrition, pharmacy, or other professionals responsible for maternal and child care. SMA LF® is a lactose-free milk based formula for babies and young children who are intolerant to lactose or sucrose, or who are experiencing symptoms such as diarrhoea, tummy ache or wind caused by temporary lactose intolerance. It is suitable as the sole source of nutrition up to 6 months of age, and in conjunction with solid food up to 18 months of age.
• The following products must be used under medical supervision.
• SMA® Comfort is a special formula intended for the dietary management of bottle-fed babies with colic and constipation. It is suitable as the sole source of nutrition up to 6 months of age, and in conjunction with solid food up to 12 months of age.

• SMA® Anti-Reflux is a special formula intended for the dietary management of bottle-fed babies when significant reflux (regurgitation) is a problem. It is suitable as the sole source of nutrition up to 6 months of age, and in conjunction with solid food up to 12 months of age. If the baby’s reflux does not improve within 2 weeks of starting SMA® Anti-Reflux, or if the baby fails to thrive, the family doctor should be consulted. • SMA High Energy® is a milk based formula for the dietary management of babies and young children with medically determined high energy requirements as identified by a healthcare professional. It is suitable as the sole source of nutrition up to 6 months of age, and in conjunction with solid food up to 18 months of age. SMA High Energy® is not intended for use with preterm babies, for whom fortified breast milk or a low birthweight formula such as SMA Gold Prem® 1 is more appropriate. DENWHS016-2;

NLNWO31-2; DENWHSP257; DSHL003-1 ZRI970_03_23 FOR HEALTHCARE PROFESSIONAL USE ONLY
Trusted to help manage symptoms of feeding issues, including functional gastrointestinal disorders (FGIDs).
SMA® Nutrition UK and Ireland ®Reg. Trademark Société des Produits Nestlé S.A.
DON’T LET PAIN HOLD YOU BACK
*To verify contact verify@perrigo.com
ESSENTIAL INFORMATION
Solpa-Extra 500mg/65mg Soluble Tablets contains paracetamol and caffeine. For the treatment of mild to moderate pain. Adults and children over 16 years: 1-2 tablets dissolved in water every 4-6 hours. Max 8 tablets a day. Children 12-15 years: 1 tablet dissolved in water every 4-6 hours. Max 4 tablets a day. Not suitable for children under 12 years. Contraindications: Hypersensitivity to the ingredients. Precautions: Particular caution needed under certain circumstances and medical advice sought for renal or hepatic impairment, Gilbert’s Syndrome, chronic alcoholism, glucose-6-phosphatedehydrogenase deficiency, haemolytic anaemia, glutathione deficiency, malnutrition or dehydration, the elderly, patients weighing less than 50kg. Precautions needed in asthmatic patients sensitive to acetylsalicylic acid, patients on a controlled sodium diet and with rare hereditary problems of fructose intolerance. Patients should be advised not to take other paracetamol containing products concurrently. Immediate medical advice should be sought in the event of overdose even if the patient feels well because the risk of irreversible liver damage. Excessive intake of caffeine should be avoided while taking this product. Interactions: warfarin and other coumarin, other medicines following the same metabolic pathway, cholestyramine, probenecid, chloramphenicol, metoclopramide, domperidone, sedatives, tranquilizers and some decongestants. Pregnancy and lactation: Not recommended during pregnancy and breastfeeding. Side effects: Rare: allergies. Very rare: thrombocytopenia, anaphylaxis, bronchospasm, hepatic dysfunction, cutaneous hypersensitivity reactions, very serious skin reactions, TEN, drug-induced dermatitis, SJS, AGEP, sterile pyuria. Unknown: nervousness, dizziness, neutropenia, leukopenia. Further information is available in the SmPC. Legal classification: P. PA 1186/017/001. MAH: Chefaro Ireland DAC, The Sharp Building, Hogan Place,Dublin 2, Ireland. Date of preparation: 04/2022. RRP (ex. VAT): €5.07. SPC: https://www.medicines.ie/medicines/solpa-extra-soluble-tablets-33783/smpc IRE SOL1 2022
14
CPD
60 Second Summary
Sleep plays a vital role in the maintenance of optimal physical and mental health. Unfortunately, sleep disorders are highly prevalent and approximately 10% of the adult population suffers from insomnia. Several chronic physical and mental health conditions are linked to sleep deprivation and sleep disruption. Sleeping less compared to your individual sleep need results in sleep deprivation and if the continuity of sleep is disturbed, it results in poor sleep quality and both sleep deprivation and disruption has daytime consequences. There are multiple factors that can cause sleep disruption and presence of sleep disorders is one of them.
The International classification of sleep disorders – 3rd edition (ICSD – 3) details different categories of sleep disorders and their diagnostic criteria. The most common sleep disorders are insomnia and sleep breathing disorders followed by sleep related movement disorders.
Cognitive behavioural therapy for insomnia (CBT-I) is a validated non-medication method to treat insomnia and is the first line treatment for chronic insomnia.
Pharmacological treatment should be considered if CBT-I is unsuccessful or not available or as an adjunct to CBT-I.
Pharmacists have an important role in the management of acute insomnia to prevent the progression to chronic insomnia by assessing, providing the sleep hygiene education, and managing the short-term sleep difficulties using over the counter sleep aids as deemed appropriate. Pharmacists can also aid by evaluating the symptoms and by advising on the referral pathway to each individual patient.
AUTHOR: Motty Varghese RPSGT, Sleep Physiologist

Motty completed his BSc in (Allied Health Sciences) with specialisation in Respiratory physiology in 2000. He registered with the Board of Polysomnography Technologists in the United States in 2008 after acquiring his international RPSGT certification. Motty attended training programmes in CBT-I in Circadian and neuroscience institute in the University of Oxford and completed a mini-fellowship in Behavioural Sleep Medicine from Perelman School of Medicine at the University of Pennsylvania. He worked as a Senior Respiratory and Sleep Physiologist at St. James’s Hospital from 2003 to 2018.
Motty currently manages the Sleep Therapy Clinic, a Behavioural Sleep Medicine clinic where he offers non-medication treatment for insomnia and circadian rhythm disorders, and sleep diagnostic services. Motty is a member of the Irish Sleep Society and the European Sleep Research Society.
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY - If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a
knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the
4 previous steps, log and record your findings.
Published by IPN. Copies can be downloaded from www.irishpharmacytraining.ie
Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author. Nytol has no editorial oversight of the CPD programmes included in these modules.
Management of Sleep Disorders: The Role played by Community Pharmacists in Advising, Managing, and offering OTC Treatment advice to those suffering from sleep disorders
Figure 1: Factors that cause sleep disruption.

Sleep plays a vital role in the maintenance of optimal physical and mental health. While sleep is a state elicited by the brain, its benefits reach far beyond brain health and even play a role in the maintenance of cellular homeostasis. Although the functions of sleep are still not fully understood, several studies have identified the restorative role sleep plays in learning, memory formation, mood regulation, brain health in general, peripheral body functions, immunity, cardiovascular and metabolic functions. The effect of sleep on maintaining alertness and keeping humans safe while performing safetycritical tasks (driving, working at heights, industries) is unequivocal.
It is a widely accepted fact that sleep deprivation/sleep disruption is very common with numerous physical and mental health related consequences of short and longterm nature. Sleep deprivation is when a person doesn’t get enough sleep compromising the total sleep quantity compared to his individually unique sleep need. The American Academy of Sleep Medicine recommends a sleep duration of over 7 hours. While sleep deprivation affects the quantity of sleep, sleep disruption affects the continuity of sleep, and thereby affecting the quality
of sleep. Sleep disruption can be caused by numerous factors including lifestyle, environmental factors, the presence of sleep disorders, and other medical conditions. In sleep deprivation and sleep disruption, sleep architecture is affected and will have daytime consequences. In a recent survey carried out among pharmacists in Ireland, it was reported one in four individuals approaching the pharmacist/pharmacy users had difficulty falling asleep, 20% reported multiple awakenings at night and 18% reported difficulty returning to sleep.
Pharmacists also reported the main issue which causes individuals to have sleep issues is stress and anxiety, followed by anxiety about sleep and environmental factors.
Lifestyle
Environ mental Psycho -social Sleep disorder
Medical conditions
Sleep architecture
41 CPD: Sleep
Continuing Professional Development
Disorders CPD
Figure 1: Factors that cause sleep disruption
42
CPD: Sleep Disorders
Sleep architecture
Sleep is broadly divided into two stages – non-rapid eye movement sleep (NREM sleep) and rapid eye movement sleep (REM sleep). NREM sleep is further divided into stages 1, 2 and 3 (previously stages 1, 2, 3, and 4) sleep. Stage 3 sleep is also called slow-wave sleep or delta sleep. Each stage of sleep has its own different functions. Stage 3 sleep is the most restorative type of sleep allowing for bodily tissue repair and growth and typically occurs in the first half of the night. Slow-wave sleep also plays a significant role in the formation of declarative memory by processing and consolidating newly acquired information. REM sleep occurs mostly in the second half of the night and helps you process emotional memories, which can reduce the intensity of emotions and in the formation of procedural memory, helping you to learn and remember the various steps involved in performing a particular task. While the above mentioned are some of the functions of sleep, they are not limited to that.
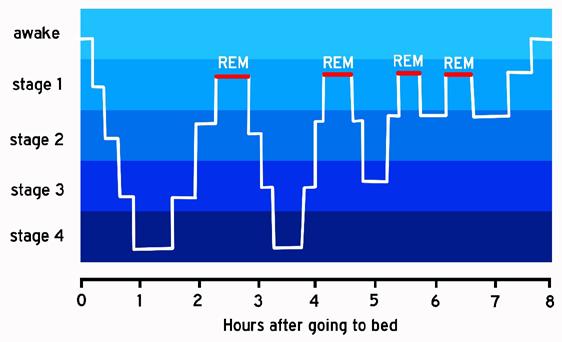
Prevalence of sleep difficulties
A Centre for Disease Control and Prevention (CDC) survey in 2014 reported that only 65% of adults reported a healthy duration of sleep, and an estimated 83.6 million adults in the United States were reportedly sleeping <7 h in 24 h.
A recent study of the prevalence of sleep disorders investigated over 20,000 patients in the Netherlands who were aged 12 years old or older found an alarming prevalence
Figure 3: Classification of sleep disorders based on ICSD-3
rate of 27.3%, with 21.2% of the males and 33.2% of the females reporting that they had some type of sleep disorder.
Insomnia is the most reported sleep disorder. The prevalence of insomnia is approximately 10% in the adult population and another 20% experiences occasional insomnia symptoms as per the research done by Prof. Charles Morin who is a professor of Psychology and eminent sleep researcher.
In a systematic review aimed at determining the prevalence of obstructive sleep apnea in adults in the general population, the prevalence ranged from 9% to 38% and was higher in men.
A survey was carried out among pharmacists in Ireland in January 2023 to understand how pharmacists experience and manage their customers’ sleep issues. More than 50% of the 240 pharmacists surveyed reported approximately 11% or more of pharmacy users consult pharmacists about sleep and 11% or more purchase sleep aids in a week, which is a clear indicator of the increased prevalence of sleep problems in this country.
INSOMNIA
SLEEP DISORDERS
CENTRAL DISORDERS OF
Other sleep disorders
• Insomnia
• Sleep-Related Breathing Disorders
Some of the sleep disorders and their general characteristics are discussed below, but the information is not exhaustive and further reading is recommended.
Sleep and mental health
Insomnia
Traditionally, sleep problems have been viewed as a consequence of mental health problems. Evidence also suggests that problems sleeping can contribute to the formation of new mental health problems and to the maintenance of existing ones. In other words, sleep has a bidirectional relationship with mental health, with problems sleeping likely to influence both the onset and trajectory of a variety of mental health difficulties.
A persistent state of anxiety, lasting for at least 6 months, is characterised as Generalised anxiety disorder. Generalised anxiety disorders are the most prevalent mental disorder among subjects complaining of insomnia. Approximately, 60% to 70% of patients with GAD also complain of insomnia.
• Central Disorders of Hypersomnolence
• Circadian Rhythm Sleep-Wake Disorders
• Parasomnias
• Sleep-Related Movement Disorders
An insomnia disorder is defined as a persistent difficulty with sleep initiation, duration, consolidation that occurs despite adequate opportunity and circumstances for sleep and concern, dissatisfaction, or perceived daytime impairment, such as fatigue, decreased irritability, general malaise, or cognitive impairment.
Sleep onset and sleep maintenance insomnia is reported widely among patients who suffer from depression. In a UK population sample, 83% of depressed patients had at least one insomnia symptom, compared with 36% who did not have depression. The association between sleep breathing disorders and depression is also well established.
In the Pharmacist Sleep Survey of 2023 (Ireland), 47% of pharmacists identify customers who may have sleep issues when they report a history of anxiety/depression.
Sleep disorders
The international classification of sleep disorders (ICSD-3) published in 2014 by the American Academy of Sleep Medicine is one of the authoritative texts for the diagnosis of sleep disorders and classifies sleep disorders into seven major categories.
A Centre for Disease Control and Prevention (CDC) survey2 in 2014 reported that only 65% of adults reported a healthy duration of sleep, and an estimated 83.6 million adults in the United States were reportedly sleeping <7 h in 24 h.
in
of 27.3%, with
• Other sleep disorders
Some of the sleep disorders and their general characteristics are discussed below, but the list and information is not exhaustive and further reading is recommended.
Insomnia
An insomnia disorder is defined as a persistent difficulty with sleep initiation, duration, or consolidation that occurs despite adequate opportunity and circumstances for sleep and results in concern, dissatisfaction, or perceived daytime impairment, such as fatigue, decreased mood or irritability, general malaise, or cognitive impairment.
Acute insomnia is often the result of an acute source of stress and tends to last from a few days to few weeks. Once the stressful period is over, sleep tends to return to normal. The annual incidence of acute insomnia in the UK is between 31.2% and 36.6%.
 Figure 2: Hypnogram depicting the sleep architecture in a normal sleeper
Figure 2: Hypnogram depicting the sleep architecture in a normal sleeper.
Figure 2: Hypnogram depicting the sleep architecture in a normal sleeper
Figure 2: Hypnogram depicting the sleep architecture in a normal sleeper.
Prevalence of sleep difficulties
A recent study2 of the
of
who were aged 12 years old or older
an alarming
21.2% of the males and 33.2% of the females reporting that they had some type of sleep disorder • Parasomnias • Sleep-Related
•
prevalence
sleep disorders investigated over 20,000 patients
the Netherlands
found
prevalence rate
Movement Disorders
Other sleep disorders
SLEEP BREATHING DISORDERS
PARA SOMNIAS
HYPER SOMNOLENCE
CIRCADIAN RHYTHM DISORDERS
SLEEP RELATED MOVEMENT DISORDERS
Figure 3: Classification of sleep disorders based on ICSD-3
Some individuals can develop perpetuating factors including maladaptive behaviours and dysfunctional beliefs and this results in insomnia lasting for a longer period and becoming chronic. The essential feature of chronic insomnia disorder is frequent and persistent difficulty initiating or maintaining sleep that lasts at least 3 months and results in general sleep dissatisfaction or perceived impairment, reported by the patient or a caregiver.
Management of insomnia
The pharmacist is in a unique position to assist with the assessment and management of acute insomnia since pharmacists are the professionals who are contacted at the beginning of sleep difficulties, often to resolve the sleep difficulty while the individual is in the pursuit of obtaining ‘over-the-counter’ medications. A thorough assessment is mandatory to establish the nature of sleep difficulty to confirm insomnia and the duration of the symptoms to confirm its acute nature.
Management should include sleep hygiene education to correct the maladaptive behaviours they may have already developed. For instance, a tendency to compensate for lost sleep by waking up late or going to bed
early, or taking long naps is very common and this can result in worsening of their insomnia. Sleep education is of paramount importance to encourage the individual to adopt optimal sleep habits. These optimal sleep habits will help them to optimise their homeostatic sleep drive and enable them to sleep better.
Pharmacological intervention in the form of non-prescription, over-the-counter sleep aids is widely used in the treatment of acute or short-term insomnia. It is the decision of the pharmacist to use OTC sleep aids depending on their efficacy and safety based on the currently available data. The dosage and duration of administration should be closely monitored.
Diphenhydramine is one of the commonly used over-the-counter sleep aids. Diphenhydramine has sedative qualities and caution should be exercised when it is provided to someone who engages in safety-critical tasks due to the residual sleepiness it may cause. It is also not generally recommended for use in older adults due to the risk of fall and other undesired effects.
Cognitive Behavioural Therapy for Insomnia (CBT-I) is recommended as the primary intervention in individuals with Insomnia as per
the Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline. Medications for chronic insomnia disorder should be considered mainly in patients who are unable to participate in CBT-I, who still have symptoms despite participation in such treatments, or, in select cases, as a temporary adjunct to CBT-I.
The following clinical algorithm is recommended for the management of Insomnia by the European guideline for the diagnosis and treatment of insomnia. (See figure 4)
Sleep breathing disorders
Obstructive sleep apnoea syndrome (OSA) is characterised by repetitive episodes of upper airway obstruction that occur during sleep, usually associated with a reduction in blood oxygen saturation or brief microarousals from sleep.
OSA is characterised by loud snoring or brief gasps that alternate with episodes of silence that usually lasts 20 to 30 seconds. Patients are usually unaware of the loud snoring and breathing difficulty or of the frequent arousals and brief awakenings that occur throughout the night and it is often the bed
diagnosis and treatment of insomnia
partner who reports the difficulty. The obstruction during sleep is mostly caused by nasopharyngeal anomalies that narrow the upper airway. Although obstructive sleep apnoea syndrome is frequently connected with obesity, some patients with this condition are not overweight; severe obesity is only found in a minority of patients. The likelihood of craniofacial anomalies like micrognathia or retrognathia is higher in the absence of obesity. Excessive daytime sleepiness is another classic feature of obstructive sleep apnoea and requires evaluation, diagnostic testing, and management by a Respiratory/Sleep specialist.
Parasomnias
Parasomnias are disorders characterised by the occurrence of complex motor or behavioural events or experiences at the onset of sleep, during sleep or during arousal from sleep. During parasomnia events, abnormal sleep-related complex movements, behaviours, emotions, perceptions, dreams and autonomic nervous system activity may occur which are potentially harmful and can cause injuries (also to the bed partner), sleep disruption, adverse health consequences and undesirable psychosocial effects. They are divided into NREM-related parasomnias, REM-related parasomnias, and other parasomnias. Confused arousals, sleepwalking, sleep terrors, sleep-related eating disorder and disorders of arousal are examples of NREM-related parasomnias. NREM sleep includes stages 1,2 and 3 of sleep and REM sleep is rapid eye movement sleep where dreams occur. REM-related parasomnias include REM sleep behaviour disorder, recurrent isolated sleep paralysis, and nightmare disorder. Examples of other parasomnias include exploding head syndrome, sleep enuresis, and sleep-related hallucinations.
Sleep related movement disorders
The most reported sleep-related movement disorders are restless
43
Clinically significant impairment? Yes Yes Yes Yes No No No No Sleep pattern in synchrony with circadian rhythm? Intake of substances that affect sleep? Change of medication Abstinence Withdrawal Treatment of comorbid disorder AND insomnia Comorbid somatic or mental disorders Psychoeducation, prevention Treatment of insomnia with CBT-I as first-line option Short-term mediactions: BZ, BZRA, sedating antidepressants Patient with sleep onset and/or sleep maintenance disturbance/early morning awakening and associated daytime impairment
Figure 4: Clinical algorithm for the
44 CPD: Sleep Disorders
legs syndrome (RLS), periodic limb movement disorder, and bruxism. Sleep disruption or daytime fatigue/sleepiness is needed for the diagnosis of a sleep- related movement disorder.
The common symptoms of RLS are an urge to move the legs usually accompanied by an unpleasant sensation in the legs that begin or worsens during periods of rest or inactivity and is partially or totally relieved by movement. These symptoms occur predominantly or exclusively in the evening or night rather than during the day. The predisposing and precipitating factors for RLS are iron deficiency, medications, pregnancy, chronic renal failure, and prolonged immobility.
Periodic limb movement can occur during sleep or wakefulness, and they should be accompanied by a complaint or objective sleep disturbance to be considered a disorder. A polysomnography (an overnight sleep test) should show a movement frequency of >15/hour in adults and >5/hour in children. PLMs can cause clinically significant sleep disturbance and when the PLMs are not explained by another current sleep disorder, medical, mental, or neurological disorder, a diagnosis of PLMS is considered.
Bruxism is characterised by cranial muscle involvement, with clenching or grinding of the teeth and/ or by bracing or thrusting of the mandible. Typically, sleep bruxism is characterised by tooth-grinding sounds and results in abnormal tooth wear, tooth pain, jaw muscle pain, and temporal headache.
Circadian rhythm sleep-wake disorders
Circadian rhythm disorders share a chronic or recurrent pattern of sleep-wake rhythm disruption primarily due to the mismatch between the endogenous circadian timing system and the sleep-wake schedule desired or required by an individual. In circadian rhythm disorders, an individual may find it difficult to maintain their major sleep phase aligned to the socially acceptable sleep phase. Some common circadian rhythm disorders are delayed sleep phase disorder, advanced sleep phase disorder, Shift work disorder and Jet lag disorder.
Delayed sleep phase disorder (DSPD) is characterised by the delay of the sleep-wake timing.
The delay is usually longer than 2 hrs and with difficulty in falling asleep at a socially acceptable time. This can result in a reduction of sleep duration and can affect the individual’s academic performance or professional life. The predisposing and precipitating factors for this disorder are evening chronotype (night owl), adolescent age, inappropriate light exposure, etc.
In advanced sleep phase disorder (ASPD), a habitual advance of the major sleep episode happens with sleep onset and final awakening happening by at least 2 hours earlier than the desired/socially acceptable time. ASPD is generally seen in older individuals, and who have a significant tendency towards morningness.
Central Disorders of Hypersomnolence
The primary complaint in the disorders included in this group is the inability to stay awake and alert during the major episodes of wakefulness during the day, resulting in periods of irresistible sleep or involuntary bouts of drowsiness or sleep. Daytime sleepiness should not be caused or explained by disturbed nocturnal sleep or altered circadian rhythms. Sleep disorders in this group include narcolepsy type 1 and 2, idiopathic hypersomnia, kleine-levin syndrome, hypersomnia due to medications, substance, or due to a medical or psychiatric disorder and insufficient sleep syndrome.
Assessment and management of sleep-related complaints
Pharmacists are in a suitable position to play an appropriate and vital role to identify sleep difficulties and improve sleep health management. Among the sleep disorders mentioned above in the ICSD – 3 classifications, Insomnia is one of the sleep disorders that Pharmacists can be of assistance and timely intervention is useful to prevent the progression of acute insomnia to chronic insomnia.
Assessment tools like, the Epworth Sleepiness scale, sleep diary to establish baseline sleep patterns, Global sleep assessment questionnaire, and sleep disorder symptom check- list are all valid tools to assess sleep health to decide on referral and further management. Careful evaluation is mandatory in identifying the symptoms and
advising the referral pathway to the concerned individual/patient. Excessive daytime sleepiness or fatigue is a common symptom in most sleep disorders due to sleep disruption (multiple awakenings) and sleep deprivation. A thorough evaluation by a specialist is warranted to identify the causal factors of sleep disruption. Full polysomnography (PSG), a diagnostic test that looks at a number of physiological variables (EEG, EMG, ECG, respiratory and abdominal efforts, oronasal airflow, SpO2, and limb movements) is required in the diagnosis of sleep disorders. Other investigations like multiple sleep latency tests or maintenance of wakefulness tests are helpful in the evaluation of central disorders of hypersomnolence in addition to the PSG but are not limited to that. Sleep diaries and actigraphy measurements are useful in the evaluation of individuals with Insomnia and circadian rhythm disorders. A referral to a sleep specialist or a respiratory physician (in the case of a suspected sleep breathing disorder) is mandatory for evaluation and further management.
Pharmacists can be resourceful for patients in the management of acute insomnia by providing sleep hygiene education and over the counter sleep aids. It is the decision of the pharmacist to use OTC sleep aids depending on individual suitability, their efficacy and safety based on the currently available data. The contraindications, dosage and duration of administration should be closely monitored.
Cognitive behavioral therapy for insomnia (CBT-I) is the first line treatment option for chronic insomnia and pharmacological treatment is generally considered when CBT-I is not successful or unavailable. Medications are also used as a temporary adjunct to CBT-I. CBT-I is delivered by a Behavioral Sleep Medicine Practitioner (Sleep Therapy Clinic www.sleeptherapy.ie).
Summary
The prevalence of sleep disorders is high in the modern industrialised society with multifaceted health consequences and impacts on individuals’ quality of life. Treating and preventing sleep disorders will have a significant impact on physical and mental health-related outcomes and pharmacists are in a unique position to contribute.
Assessing and managing insomnia and educating individuals about sleep hygiene during the early phase using evidence-based methods helps to prevent the progression of it to a chronic condition. Identifying the symptoms of other sleep disorders and advising individuals on the referral pathway to resolve their sleep difficulty is another area where pharmacists can be resourceful.
Recommended reading:
Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline.
International classification of sleep disorders – 3rd edition (ICSD – 3) References available on request
Question your Understanding
1. What is ICSD - 3 and what are the different types of sleep disorders?
2. What is the difference between acute insomnia and chronic insomnia and who can be treated in the pharmacy?
3. What are the nonmedication methods to treat insomnia?
4. What are the common sleep disorders, and do you know the symptoms of them to identify and refer to a GP or a specialist?
5. What are the factors that cause sleep disruption?
IREL AND’S No.1
Sl eep A Id BRAND CAN H E LP YOU GET A GOOD NIGHT’S SLEEP
*Based on IQVIA sales data MAT 07/2022.
CLINICALLY PROVEN
Nytol One-A-Night 50 mg Tablets contains diphenhydramine hydrochloride. A symptomatic aid to the relief of temporary sleep disturbance in adults. Adults: One tablet to be taken 20 minutes before going to bed, or as directed by a physician. Do not exceed the maximum dose of one tablet in 24 hours. Elderly patients or patients with liver or kidney problems should consult their doctor before taking this medicine. Children under 18 years: Not recommended. The product should not be taken for more than 7 days without consulting a doctor. Contraindications: Hypersensitivity to the active substance or to any of the excipients, stenosing peptic ulcer, pyloroduodenal obstruction, phaeochromocytoma, known acquired or congenital QT interval prolongation, known risk factors for QT interval prolongation. Special warnings and precautions: Pregnancy/lactation, renal and hepatic impairment, myasthenia gravis, epilepsy or seizure disorders, narrow-angle glaucoma, prostatic hypertrophy, urinary retention, asthma, bronchitis, COPD. Patients should be advised to promptly report any cardiac symptoms. Tolerance and / or dependence may develop with continuous use. Do not take for more than 7 consecutive nights without consulting a doctor. Should not be used in patients currently receiving MAO inhibitors (MAOI) or patients who have received treatment with MAOIs within the last two weeks Use in the elderly should be avoided. Avoid concomitant use of alcohol or other antihistamine-containing preparations. Do not drive or operate machines. Cases of abuse and dependence were reported in adolescents or young adults for recreational use and/or in patients with psychiatric dis-orders and/or history of abuse disorders. Contains lactose. May suppress the cutaneous histamine response to allergen extracts and should be stopped several days before skin testing. Interactions: Alcohol, CNS depressants, MAO inhibitors, anticholinergic drugs (e.g. atropine, tricyclic antidepressants), metoprolol and venlafaxine, CYP2D6 inhibitors, Class Ia and Class III anti-arrhythmics. Side effects: Dry mouth, fatigue, sedation, drowsiness, disturbance in attention, unsteadiness, dizziness, thrombocytopenia, hypersensitivity reactions, confusion, paradoxical excitation, convulsions, headache, paraesthesia, dyskinesias, blurred vision, tachycardia, palpitations, thickening of bronchial secretions, gastrointestinal disturbance, muscle twitching, urinary difficulty, urinary retention. Legal classification: P. PA1186/016/001. MAH: Chefaro Ireland DAC. The Sharp Building. Hogan Place. Dublin 2. Ireland. Date of preparation: 07/2022. RRP (ex. VAT): 20s €9.00. SPC: https://www.medicines.ie/medicines/nytol-one-a-night-50-mg-tablets-34889/smpc IRE NYT

2022 18
Irish Pharmacy Awards 2023
Ireland’s ‘Most Trusted’* pharmacy publication - Irish Pharmacy News - are delighted to announce the launch of the annual Irish Pharmacy Awards 2023
Now is the time to recognise that dedication.
The Irish Pharmacy Awards 2023 will be a celebration of success and also a platform of gratitude to community pharmacists and their teams. The awards recognise excellence and innovation and this is the premier opportunity for the industry to show their appreciation.
We look forward to welcoming you all to Clayton Hotel, Burlington Road, Dublin on
Entries are now open:
Haleon Self-Care Award
United Drug Business Development (Independent) Award

Perrigo Superintendent Pharmacist of the Year

Reckitt Community Pharmacist of the Year


Uniphar Category Development of the Year Award


JPA Brenson Lawlor Young Community Pharmacist of the Year Award
Points of Care Testing Pharmacy of the Year Award
Recognising the importance of continued knowledge, education and sharing of information amongst the pharmacy profession Closing Date for Entries: March 31st, 2023 For an Entry Form Contact: Aoife Jackson on: Mobile: 00353 (87) 337 9258/07444757673 Email: aoife@ipn.ie
BOI Payment Acceptance (BOIPA) Innovation & Service Development (Chain) Award
Viatris Community Pharmacy Team of the Year Award
McLernons Independent Community Pharmacy of the Year Award
Théa Pharma OTC Counter Assistant of the Year Award

Community Pharmacy Technician of the Year Award
Easolief DUO Business Development (Chain) Award
BOOK YOUR TABLE
Over 650 of Ireland’s pharmacy industry professionals will join us on Saturday, May 27th 2023 at the Clayton Hotel (Burlington Road) Dublin. Don’t miss out on this opportunity to network and celebrate community pharmacy. This is sure to be a night to remember. Seats and tables are filling up fast. Book your table now to attend Ireland’s premier Pharmacy Awards event. Contact Aoife Jackson via email: aoife@ipn.ie
Introducing... MGK9299 Haleon Trade Ads.pdf 10/08/2022 14:58
Community Pharmacy Technician of the Year 2023
It is evident that pharmacy technicians are playing an increasingly important supporting role as pharmacists are increasingly spending more time with patient consultations and engaging local stakeholders.
The shift in emphasis from dispensing to healthcare provision has meant that the wider pharmacy team has to pull together – pharmacy technicians capture the essence of this in everything that they do.
The Community Pharmacy Technician of the Year Award will recognise the winner’s important contribution to the community pharmacy technician profession. Applications are invited from both the independent and chain sectors.

How to Enter:
The judges will be looking for those who can demonstrate promotion of the role ofthe Pharmacy Technician and those who continue to champion excellence through forward thinking and innovation.
The winners’ achievements will be an inspiration to those pursuing innovative practice; to those striving to raise standards; and to pharmacists who, through their professionalism, provide models for others within pharmacy.

Awards Criteria:
1. Evidence of long-term, consistent dedication and outstanding achievements that have led to the advancement of the profession of pharmacy and public health
2. Evidence of a large variety of skills, attributes and accomplishments
3. Evidence of an individual strong in character, cumulative professional accomplishments and the ability to properly represent and model what pharmacy technicians as a profession encompasses
4. Evidence of an understanding the goals of pharmacy, and significantly contributing to how these goals may be achieved
PHARMACYNEWSIRELAND.COM | 47
Applications Close - March 31st, 2023 Send your entries to - aoife@ipn.ie Download application forms from: https://irishpharmacyawards.ie/
Théa Pharma OTC Counter Assistant of the Year Award 2023
Pharmacists are widely recognised for their invaluable work in the community. But what about the rest of the team? All of the team and especially the counter staff play a critical role in the success of the pharmacy and the service it provides.
Perhaps you are a counter assistant, or know of one who has made a huge impact within their local pharmacy around customer care, delivering health promotion activities or forging links with the local community. Or you/they might have improved safety or efficiency in the dispensing process, taken on delivery of clinical services or management responsibilities, or mentored colleagues.
How to Enter:
The Théa Pharma OTC Counter Assistant of the Year Award recognises excellence in knowledge and service to retail customers. Nominations for the category can be made through self-nomination, by colleagues or by pharmacy business owners.


Judges will be looking to reward those who bring something extra to the consumers experience of the pharmacy setting within a community.
Awards Criteria:

1. Clear demonstration of how the nominee/counter assistant has successfully placed customer care at the forefront of their pharmacy
2. The details and rationale for any specific initiatives developed by the nominee for customer care
3. Levels of excellence displayed above and beyond that expected from a counter assistant role
4. Clear evidence of team working and excellent communication between the individual, their peers/colleagues and their patients and local community
48 | PHARMACYNEWSIRELAND.COM
BOI Payment Acceptance (BOIPA) Innovation & Service Development (Chain) Award 2023
* Open to all pharmacies with more than 3 stores
The Innovation & Service Development Award’s principal aim is to reward innovation within the community pharmacy sector. The judging panel will be looking for ways in which a project is both innovative and successful.
This Award identifies individuals and teams working within multiple community pharmacies in Ireland whose ideas or inventions have, or could lead to, improvement in the patient experience in all areas of care throughout their community.

How to Enter:
Applications are sought from those demonstrating clear enthusiasm and commitment to the enhancement of community pharmacy in Ireland, exceptional quality above and beyond what is expected and an ability to overcome challenges in pursuit of goals.
Awards Criteria:
1. Activities that may involve pioneering new models or systems that improve pharmacists’ impact as members of the healthcare team; patient safety and outcomes; patient care in general and other professional development
2. Development of a system or tool for pharmacy that will directly or immediately impact patient care or the profession and/or serve as an example or template for other pharmacy professionals to follow
3. Measurable benefits of your initiative. Please use financial data wherever possible (percentages, rations, graphic images etc.), as well as other statistics to show how your project has bought added value, profits, customer satisfaction improvements, productivity increases or any other benefit relevant to this award category.
Applications Close - March 31st, 2023 Send your entries to - aoife@ipn.ie
Download application forms from: https://irishpharmacyawards.ie/

PHARMACYNEWSIRELAND.COM | 49
United Drug Business Development (Independent) Award
2023
The United Drug Business Development (Independent) Award serves to recognise those who have displayed success in terms of sales, training, recruitment, customer service, product development or other areas of business development.

Entries should demonstrate an innovative approach to creating new business, and outline the timescales, objectives and results of the initiative.
How to Enter:
Judges will look for a business initiative that stands out in terms of its scale, scope or approach. This award will credit the company that has demonstrated excellent levels of customer service backed by clear standards and adequate monitoring performance.
Awards Criteria:

1. Clear demonstration of an identified need and personal rationale along with details of the process of implementation from concept to design, planning and results
2. Evidence will be displayed for plans for further research and development
3. Evidence of a sound business plan, sales and marketing strategies
4. Strong leadership skills with the ability to drive the business forward Innovation and ambition
50 | PHARMACYNEWSIRELAND.COM
* Open to all pharmacies with less than 3 stores
Easolief Duo Business Development (Chain) Award 2023
The Esolief Duo Business Development (Chain) Award serves to recognise those who have displayed success in terms of sales, training, recruitment, customer service, product development or other areas of business development.

Entries should demonstrate an innovative approach to creating new business, and outline the timescales, objectives and results of the initiative.
How to Enter:
Judges will look for a business initiative that stands out in terms of its scale, scope or approach. This award will credit the company that has demonstrated excellent levels of customer service backed by clear standards and adequate monitoring performance.
Awards Criteria:
1. Clear demonstration of an identified need and personal rationale along with details of the process of implementation from concept to design, planning and results
2. Evidence will be displayed for plans for further research and development
3. Evidence of a sound business plan, sales and marketing strategies
4. Strong leadership skills with the ability to d rive the business forward Innovation and ambition
Applications Close - March 31st, 2023 Send your entries to - aoife@ipn.ie
Download application forms from: https://irishpharmacyawards.ie/
PHARMACYNEWSIRELAND.COM | 51
* Open to all pharmacies with more than 3 stores
McLernons Independent Community Pharmacy of the Year Award 2023
This is a New Award Category for 2023, open to all pharmacies with 3 or less stores. The McLernons Independent Community Pharmacy of the Year Award seeks to recognize excellence within the independent community pharmacy sector.
Independent pharmacies across Ireland have long been the backbone of community services, but must continuously look for new ways to be innovative, delivering high quality patient care and pharmacy offerings to rival the increasingly competitive force of the larger multiples and chain stores.
The judging panel will be looking for ways in which entries are both innovative and successful.
This Award identifies pharmacy stores and their teams who have demonstrated dedication towards their customer-base in all areas of care throughout their community.
How to Enter:
Applications are sought from those demonstrating clear enthusiasm and commitment to the Independent community pharmacy business in Ireland, exceptional quality above and beyond what is expected and an ability to overcome challenges in pursuit of goals.
Awards Criteria:
1. Measurable benefits your pharmacy has brought to the community; with evidence to show how you have brought added services or value to your customers; productivity increases or other benefits relevant to this Award
2. Evidence of strong team working, clear goals and achievements
3. Demonstration of how your independent pharmacy has had an impact on the community its serves
4. Evidence of how your way of working, within an independent, rivals the larger multiple stores to bring the same benefits to patients
52 | PHARMACYNEWSIRELAND.COM
Haleon Self-Care Award 2023






The Haleon Self-Care Award recognises community pharmacy’s commitment to tackling health inequalities and serves to reward achievement in the development and implementation of health promotion, self-care and community wellbeing strategies/initiatives.
It is designed to encourage excellence in the production and dissemination of accessible, well-designed and clinically balanced patient support.
How to Enter:
The Award will be presented to the team or individual who can demonstrate a significant positive impact on the experience of those who use Pharmacy services. This may be through campaigns, promotions or initiatives which have identified a need within the community to address certain health issues.
Awards Criteria:






1. Evidence of long-term, consistent dedication and outstanding achievements that have led to the advancement of the profession of pharmacy and self-care








2. Evidence of how you/your team have researched and identified a need within the self-care market and how you have met this need for the enhancement of patient care
3. Examples of entries may include evidence of the impact your self-care offering has had on the community you serve/ improved your links with allied healthcare professionals or organisations and/or tackled a health inequality through self-care initiatives and promotions
Applications Close - March 31st, 2023 Send your entries to - aoife@ipn.ie
Download application forms from: https://irishpharmacyawards.ie/

PHARMACYNEWSIRELAND.COM | 53
Introducing...
MGK9299 Haleon Trade Ads.pdf 1 10/08/2022 14:58
Haleon, formerly part of GSK
Uniphar Group Category Development Award 2023
The Uniphar Group Category Development Award aims to recognise the specialist knowledge and expertise of pharmacies in areas such as first aid, derma skincare or vitamins, minerals and supplements.

Running a successful pharmacy means much more than knowledge of top-selling products. The ability to optimise retail performance through a specific group of products managed as a distinct business unit shows an understanding and appreciation of the market and the ability to excel in these competitive times.
How to Enter:
Judges of this category will be looking for an identified need within the pharmacy, followed by details of the project implementation process from conception to resolution.
The Award is seeking entries from those who can demonstrate the measurable benefits from a specific project or initiative and have added value, profits, increased productivity and customer satisfaction.
Awards Criteria:
1. Evidence of training, education and/or support initiatives undertaken by the pharmacist/pharmacy team
2. Demonstration of benefits from a specific project
3. Examples of fresh thinking within category development for the enhancement of this sector within community pharmacy
4. Ambition in improving performance, furthering knowledge and understanding of the market
54 | PHARMACYNEWSIRELAND.COM
OTC Retailer of the Year Award 2023
Customer purchases of OTC products have consistently risen, for many reasons. The convenience of treating a condition with an OTC product is appealing to the typically busy person, who seeks to avoid a lengthy and expensive GP visit in favour of meeting the demands of home and work. In addition, patients in the information age have an increased level of awareness about health.
The over-the-counter market continues to thrive as manufacturers continue to think of new promotional and packaging ideas and as the general public take a greater interest in their own health and wellbeing. Pharmacies are increasingly witnessing heightened footfall as GP visits decrease
Pharmacy staff are the focal point for helping customers select appropriate OTC medicines, suggest diagnostic testing and accessory products and must be aware of when to refer individuals to the pharmacist. Knowledge of the market is essential; seasonal products and accessories; the use of displays and front of shop expertise and judges will want evidence of excellent merchandising strategies.
How to Enter:
Judges will look for a pharmacy business, either independent or multiple, that stands out in terms of their OTC retail offering, whether this be through the introduction of new initiatives, growth of scale, scope or approach. This Award will credit the pharmacy that has demonstrated excellent levels of customer service backed by clear standards and adequate monitoring performance across the OTC market.
Awards Criteria:
1. Demonstration of identifying key promotional opportunities to add value for the customer such as health promotion events and displays
2. A showing of continuous working with manufacturers and suppliers to plan yearly promotional calendars to meet pharmacy profit goals
3. Implementation of innovative strategies to competitive pricing
4. Examples of education for staff on new products and convenyance tocustomers as to efficacy and usage
Applications Close - March 31st, 2023 Send your entries to - aoife@ipn.ie
Download application forms from: https://irishpharmacyawards.ie/
PHARMACYNEWSIRELAND.COM | 55
Perrigo Superintendent Pharmacist of the Year 2023

Superintendent pharmacists have overall responsibility for setting out the standards and policies for the provision of pharmacy services by their organisations. The role of Superintendent Pharmacist is a key position carrying full time responsibility and accountability.
This Award will be looking to recognise those individuals who are serving as key drivers for the implementation of enhanced and excellent pharmacy care within the community they serve. Judges will be looking for applications from those that are focused on establishing a framework for achievement of a high quality, safe and consistent service for the benefits of the patient, as well as facilitating the development of the professional role of the pharmacist.
How to Enter:
Judges will be looking for applications from those that are focused on establishing a framework for achievement of a high quality, safe and consistent service for the benefits of the patient, as well as facilitating the development of the professional role of the pharmacist.
Awards Criteria:
Applications are invited from independent and multiple Superintendent Pharmacists who can demonstrate one or more of the following:
1. Understanding patient needs when delivering healthcare in the community
2. Examples of great patient experience and care, innovation and ambition
3. Best practice in delivering professional services and patient reviews
4. Encouragement of staff education in patient health and wellbeing advice
5. Strong leadership skills with the ability to drive the business forward
56 | PHARMACYNEWSIRELAND.COM
JPA Brenson Lawlor Young Community Pharmacist of the Year Award 2023
The JPA Brenson Lawlor Young Community Pharmacist of the Year Award recognises rising talent – those individuals who despite being in the early stages of their pharmacy careers are already demonstrating that they can make a difference to the pharmacy profession and the companies for whom they work and the communities they serve.
How to Enter:
This award is open to pharmacists aged up to 30 - at the date of entry submission - who are working within any pharmacy, multiple or independent, where their involvement has been greater than six months.
It is the individual qualities that will be evaluated, rather than those of any of the projects worked on.
Awards Criteria:
1. Judges will want to see effective communication skills with both staff and customers
2. Demonstration of a commitment to mentoring or other leadership activities
3. Operation within their own pharmacy liaising with key staff members and management and developing key communication skills
4. A dedication and commitment to furthering the profession into the future
Applications Close - March 31st, 2023 Send your entries to - aoife@ipn.ie
Download application forms from: https://irishpharmacyawards.ie/
PHARMACYNEWSIRELAND.COM | 57
Reckitt Community Pharmacist of the Year 2023

The Reckitt Community Pharmacist of the Year Award seeks to recognise a community pharmacist who is defining the future standard of pharmacy practice by his or her professional practice and/or by advocacy in the pharmacy industry.
Judges will be looking for those who demonstrate leadership and exemplifies the evolution of the pharmacy profession towards an expanded role in health care. The winner will be able to show significant contributions to the pharmacy industry overall resulting in meaningful improvements in the quality of patient care and improved delivery models and pharmacy’s role on the health care team. Applications are invited from both the independent and chain sectors.
How to Enter:
To be eligible, a nominee must have been practicing for at most 5 years. Those working under the age of 30 should apply for the Young Community Pharmacist of the Year category.
Awards Criteria:
1. Evidence of long-term, consistent dedication and outstanding achievements that have led to the advancement of the profession of pharmacy and public health
2. Evidence of a large variety of skills, attributes and accomplishments
3. Evidence of an individual strong in character, cumulative professional accomplishments and the ability to properly represent and model what pharmacy as a profession encompasses
4. Evidence of an understanding the goals of pharmacy, and significantly contributing to how these goals may be achieved
58 | PHARMACYNEWSIRELAND.COM
Viatris Community Pharmacy Team of the Year Award 2023
This Award will be given to the community pharmacy team that demonstrates the best combination of team spirit and enhancement of patient care at all levels.
The judges will be looking for those who encourage and support each other and those who have collectively demonstrated innovation and forward thinking.
How to Enter:
The key to any successful pharmacy is Teamwork and this award recognises the power and potential of a focused and unified approach to healthcare initiatives. Teams can be based within one organisation or spread over multiple organisations; but they must comprise individuals working towards the same objective or goal.
Awards Criteria:
1. How the team has demonstrated their ability to deliver clear benefits to patients; and/or staff members through working together efficiently and effectively
2. How the team has worked together to achieve its objectives over the past twelve months
3. Projects that the team has successfully managed which demonstrate excellence in quality, innovation, productivity and prevention
4. A clear display of the principles underpinning their success as a team
Applications Close - March 31st, 2023 Send your entries to - aoife@ipn.ie
Download application forms from: https://irishpharmacyawards.ie/
PHARMACYNEWSIRELAND.COM | 59
Management of Menopausal Skin
 Written by Dr. Laura Lenihan, Skin Expert, GP & Aesthetic Doctor at Dr. Laura Clinic, Galway and Dr. Kate Gilmore, Dr. Laura Clinic, Galway
Written by Dr. Laura Lenihan, Skin Expert, GP & Aesthetic Doctor at Dr. Laura Clinic, Galway and Dr. Kate Gilmore, Dr. Laura Clinic, Galway


Clinical presentation
With female adult acne, there are 2 subtypes now recognised. Persistent adult acne, which is defined as acne that persists beyond adolescence and into adulthood and accounts for 80% of cases in female adult patients. And late onset acne, acne that begins after the age of 25.
Hormonal acne is often concentrated along the lower face (typical U pattern versus T pattern associated with teenage acne), with a typical pattern presenting around the jawline extending down to the neck. It can often present concurrently on the chest and back. Lesions are more often of the papulopustular or nodular kind. In practice, there do not tend to be a lot of open or closed comedones (blackheads and whiteheads) in adult female acne, which can sometimes make diagnosis difficult and can lead to missed opportunities to treat.
Acne
Acne is typically viewed as a disease of adolescence, however this common generalisation can contribute to stigma experienced by those who suffer from adult acne – broadly defined as persistent or new lesions at the age of 25 or older. Acne has been linked to a number of debilitating psychological symptoms, despite often being dismissed by clinicians as a minor condition. Many patients report increased levels of anxiety and depression, and an overall decreased quality of life that does not correlate necessarily with severity of disease.
Hormonal acne can be particularly difficult to treat as it is often approached by patients and clinicians with the same methods used to treat adolescent acne. To understand why it requires an alternative approach, it is important to first understand the pathophysiology of the disease.
Pathogenesis
Acne is a disease of the pilosebaceous unit, or the pore. The pathogenesis of acne is broadly considered to consist of four elements: hyperkeratinization of pilosebaceous follicles, followed by excess sebum production (worsened by hormones), c. acnes
colonisation and inflammation. C. acnes, a bacteria found in pilosebaceous follicles, has been shown to induce an inflammatory response which promotes follicular rupture. By promoting sebaceous gland growth and secretory activity, androgens contribute to acne formation. Androgen levels also don’t have to be abnormal, or high, but rather the androgen receptors in the pores respond inappropriately to normal levels of hormones. Within the realm of female adult acne, androgens play a major role. Hyperandrogenism, such as PCOS is an important factor to be aware of and clinicians should be advised to look out for signs of PCOS such as hirsutism and irregular periods. If a patient has signs of hyperandrogenism and late onset acne then they should be further evaluated for an underlying endocrine disorder such as PCOS with their GP.
Contributing factors
We do know that there can be a variety of contributing factors but how much of a role they have to play is very much still up for debate. These include genetics, diet (mainly high GI foods like dairy products and chocolate), environmental factors, stress and occlusive cosmetics.
Other common presentations would be patients experiencing acne for the first time since their adolescence after discontinuing birth control pills, patients who are perimenopausal, and patients who experience the worst flare ups during their periods. Pregnant patients can also present with flare ups.
Treatment
Hormonal acne can be particularly challenging for patients as it is seemingly resistant to conventional first or second line acne treatments. Often a patient will present having tried numerous forms of topical treatments which proved effective in their youth are
now doing very little to combat their symptoms.
When it comes to treatment, it’s important to remember the pathogenesis and ensure that we treat all four of the major issues. Treatment can be challenging as it can have a chronic course (13-16 years for some or longer) and there can be high rates of failure and often numerous choices for the clinical. As important as treatment is, maintenance and prevention is key and so treatment should be considered for a much longer period of time. For us here in clinic, we cannot stress the importance of skincare in the treatment of adult onset acne, as it is required to alleviate lots of the issues causing acne in the first place. While medications work, tretinoin being the gold standard and working across all 4 issues, there is lots that we can do with skincare as well, using ingredients that reduce keratinisation of pores, to help decrease sebum and inflammation. WIth adult women, there are significantly higher rates of treatment failure, 80% of women will fail multiple courses of systemic antibiotics and up to 3040% of women will fail roaccutane.
Le’ts take a look at some of the treatment options
Given the role that androgens play, it’s clear that medications that affect androgen levels will have an important role in the treatment of female adult acne. This means the combined oral contraceptive pill (COCP) and spironolactone will be saviours for most patients.
The COCP works with oestrogen increasing levels of sex hormone binding globulin (SHBG), which
60
Acne & Menopause
Dr Laura Lenihan
PHARMACYNEWSIRELAND.COM
Dr Kate Gilmore
binds with excess free androgens stopping them affecting sebum levels. The COCP works well for acne lesions focused around the jaw and chin area, or if there is a history of flaring that coincides with menstrual cycles. It’s a great option for women who also need contraception. There are however a number of contraindications to the use of the COCP including, increased BMI, smoking, pregnancy, and hypertension. The GP or prescriber should advise patients of the same.
Spironolactone works by blocking the androgen receptors in the pilosebaceous unit. This results in shrinking of the sebaceous glands and a reduction in sebum production. Spironolactone is an excellent choice for patients who have tried hormonal therapies with varying results and do not wish to use isotretinoin. As spironolactone is a diuretic, it is important to advise patients to keep well hydrated by consuming the recommended 2L of fluid a day. The American Academy of Dermatology states that spironolactone can be used in patients under the age of 40 without any medical issues, without testing U+E. In any patients with a medical history they should be checked pre treatment, after initiation and with any dose changes.
Isotretinoin (brand name Roaccutane) is a Vitamin A derivative. It is the gold standard for severe and recalcitrant acne. It works by shrinking overactive oil glands and it has also been shown to reduce c. acnes in the skin.
For many patients, isotretinoin is a life changing drug, but it is not without its pitfalls. Patients will need to be counselled about numerous side effects, including dry, cracked skin – especially in mucous membranes. Over the counter lip balms with ceramides and saline nasal sprays can help to soothe these symptoms. Dry, inflamed eyes and eyelids can also be treated with various over the counter drops and gels.
Routine monitoring of liver function tests, serum cholesterol and triglycerides and regular pregnancy tests are necessary for the duration of treatment. There has been much discourse surrounding isotretinoin and its effects on mood, and it has long been associated with depression and increased risk of suicidality. Despite persistent studies, there is still little evidence to support this. Patients should be aware that they should contact their GP immediately if they notice any mood changes.
Both spironolactone and isotretinoin pose teratogenic risks so it is important to ensure that
patients are informed of these risks before starting the medication. The patient will need to be on adequate birth control. For isotretinoin two forms of contraception are recommended, with one being a barrier method. Long acting reversible contraceptives such as the coil should be considered.
Topical treatments
There are a lot of topical treatment options for acne, many of which can be very successful. However some are better for younger age groups than others. Topical treatment is also ESSENTIAL for maintenance and prevention of further lesions and should be initiated alongside any oral therapy.
Topical Tretinoin (retinoic acid) is considered the gold standard for topical therapy in acne.
It should be used over adapalene (differin) in older patients. All patients with acne can benefit from topical retinoid treatment, which are an important part of maintenance therapy. For example, in the case of severe hormonal acne which has been treated with isotretinoin, daily application of topical tretinoin can play a vital role in maintaining treatment responses following the discontinuation of isotretinoin. Tretinoin also has the advantage of significant anti-aging benefits, including increasing cell turnover, increasing collagen synthesis therefore reducing fine lines and wrinkles, and evening skin tone by decreasing pigmentation. This makes it a fantastic option in older age groups looking for anti ageing benefits as well.
Azelaic acid (Rx Skinoren) can be prescribed by clinicians but also can be found in many over the counter products. Azelaic acid is usually tolerated very well by patients, and reduces c. acnes on the skin while also decreasing keratin production and offsetting the effects of post-inflammatory hyperpigmentation. It is both an anti inflammatory and anti bacterial agent and can be used with good effect in acne. In clinic we would prescribe skinoren in the AM and tretinoin in the PM for acne treatment and maintenance. This is considered to be the gold standard among dermatologists worldwide. It is also safe to use in pregnancy and breastfeeding and so a good option for women who may otherwise struggle.
Topical antibiotics have not been found to have the best efficacy in hormonal acne. Furthermore, sustained topical antibiotic use can confer antibiotic resistance, especially when used by itself. Benzoyl peroxide, although a mainstay in adolescent acne, has

been shown to be less effective in the treatment of hormonal acne. Topical retinoids are preferable. Emphasising to patients that establishing a consistent skincare routine is the hallmark of maintaining results. If patients are using topical acne treatments that are drying or have side effects then for the most part their skincare routine should be nourishing. Look out for gentle cleansers used both AM and PM. There is no need to clean the skin more than twice per day. Ingredients such as salicylic acid can be used to decrease oil levels and unclog pores. Niacinamide is a potent anti-inflammatory agent that also works to control sebum levels and is found in a number of cosmetic products. Alphahydroxy-acids such as glycolic acid or lactic acid can be used to work on texture, reducing blockage of pores. Looking out for a non comedogenic moisturiser and SPF are also key.
Another important element of treatment is ensuring that the patient is aware of the timeline of treatment. Often breakouts can worsen in the first few months of treatment, especially with the use of topical treatments such as tretinoin. Patients should 100% be informed of the risk of purging, as many will quit therapy thinking it isn’t working. Results take a minimum of 8 - 12 weeks and often longer for more severe cases.
Two new advancements in acne therapy include the recent approvals of both the AviClear laser and clascoterone 1% topical cream. Both have shown promise in the area of hormonal acne.
Although clascoterone is not yet licensed in Ireland or the UK, its initial clinical data is promising. It acts as an androgen receptor blocker. It is a novel treatment, the first topical anti-hormonal treatment on the market. It will be especially beneficial for patients who cannot tolerate the side
effects of systemic androgen receptor blockers. It is not expected that clascoterone will be a substitute for all other therapies, but that it will be a very beneficial adjunct to current treatments. Early studies suggest it has a possible role in reducing the dosage of and even hastening the discontinuation of oral therapy. With already limited options for treating hormonal acne, this new addition to the physician’s arsenal is a very exciting one.
The AviClear laser from Cutera is a 1762nm wavelength laser which is the first device of its kind to be cleared by the FDA. The advent of machines such as the AviClear which target sebaceous glands without damaging surrounding skin could also spell a new era for acne treatment, providing an option for patients who are pregnant or who cannot tolerate certain oral or topical treatments. Initial studies have suggested that the AviClear could be as efficacious as isotretinoin at the two year post treatment mark. As the device is extremely new, having been approved in March 2022, further research will be needed to cement its status as a viable alternative to isotretinoin.
Menopausal skin
Menopause officially begins one year after your final period however many women will start to notice changes in their skin long before this while going through perimenopause. During perimenopause the body’s production of oestrogen and progesterone, the two hormones made by the ovaries, varies greatly giving symptoms such as hot flushes etc. High levels of oestrogen seen in younger women help to keep the skin healthy and plump by stimulating the production of collagen, glycosaminoglycans and natural oils. Collagen is the primary protein in skin, but also nails, hair muscles and bone. As you age and oestrogen levels drop, we see a decrease in the production
PHARMACYNEWSIRELAND.COM 61
of collagen, which means the skin becomes more susceptible to dryness and fragility. By the time a woman is postmenopausal her oestrogen production has stopped. So how does this affect skin? From dryness to rashes, menopause has many different effects on women’s skin.
The main complaints that patients will mention include: general ageing of the skin such as wrinkles and a reduction in elasticity, skin dryness and itching, acne (menopausal breakouts are quite common), increased skin sensitivity, redness associated with hot flashes, facial hair, hair thinning, as well as changes to the skin around the genital area which is highly susceptible to changes in oestrogen.
While we know the effects of oestrogen on lots of body systems, including cardiovascular; the effects it has on the skin are less well understood. We do know that it prevents a decrease in skin collagen production. From the age of 25 we lose about 1% of our collagen a year but in the first five years after menopause we lose a further 30% which can have significant changes on our skin. Oestrogen is also known to maintain stratum corneum barrier function, it increases hydration levels by increasing glycosaminoglycans and hyaluronic acid in the skin and also has an effect on elastin fibres. By removing oestrogen this can have a deleterious effect on our skin showing as dryness, thinning skin, loss of elasticity and loss of collagen. The overall effect is an increased rate of ageing. Menopause can also have an effect on the hair of both your face and scalp.
Although hormonal therapy (HRT) remains the gold standard for treating many of the physical symptoms of menopause, there is no evidence that it helps with age-related skin changes in patients who are postmenopausal. Some studies have shown however an increase in sebum
levels in postmenopausal women receiving HRT so watch this space.
Skin issues at menopause

Fine lines & wrinkles
WIth that reduction in collagen fine lines & wrinkles appear where we never had them before. They can increase substantially after menopause.
How to fix them?
SPF should be used daily to prevent further damage occurring ideally alongside a potent antioxidant serum in the AM such as L-Ascorbic Acid to negate the effects of UV damage on the skin. Retinoids (prescription retinoic acid or over the counter retinol) are great for stimulating collagen production and increasing cell turnover. Some people advocate for taking vitamin C supplements also as it is an essential precursor to the formulation of collagen.
Age spots / pigmentation
During menopause, skin becomes even more susceptible to UV damage. Concurrently, UV damage that has already accumulated below the surface of the skin can rise to the skin’s surface, causing hyperpigmentation. Many patients complain of worsening “sun spots” at the onset of menopause. Skin cancer and precancerous skin growths can also become more common. Remember UV damage is cumulative.
How to fix it?
It is vital to counsel patients on the importance of sun protection. SPF 50 should be worn daily, and patients should avoid direct sunlight as much as possible. Conservative measures such as wearing wide brimmed hats and protective clothing, staying in the shade and avoiding being outside for too long during peak sun hours in the summer months can all aid in preventing further damage and pigmentation. If a patient is worried about any spots then they should have them assessed by a GP or dermatologist and do regular self skin exams.
Other ingredients mentioned below will help with pigmentation. Alpha hydroxy acids such as lactic acid and glycolic acid will shed away dead skin cells that have extra pigment in them. Retinoids help to reduce pigmentation by blocking tyrosinase. Vitamin C and other antioxidants help to reduce the deleterious effects of UV rays on the skin. If the pigmentation is bad, we can use prescription skin bleaching products such as hydroquinone, which must be used under medical supervision.
Dry Skin
During menopause, the stratum corneum weakens and there is an increase in water loss from the skin. As oestrogen levels drop, the skin produces less sebum, hyaluronic acid and ceramides, which are all essential in keeping the skin barrier intact and preventing transepidermal water loss (TEWL).
How to fix it?
Using moisturisers containing ceramides, shea butter, fatty acids, hyaluronic acid and squalane that help to maintain the integrity of the skin barrier and keep water in, and bacteria and pollutants out. Switch to a gentle cleanser that won’t strip dry skin of its essential oils. We prefer a cream cleanser for menopausal skin rather than a foaming one.
Sensitive skin
With the onset of menopausal symptoms, many patients complain of increased sensitivity. As we age, our skin’s pH changes which can lead to increased sensitivity to products which may have previously suited our skin. How to fix it?
The most important thing is to use gentle products and see a cosmetic doctor if there is any irritation. Using pH balanced cleanser and moisturisers can also help and avoid irritating ingredients such as glycolic acid while you improve the overall structure and function of skin.
Dullness
As we age, the rate at which we turn our cells over decreases leading to dullness (old cells that don’t reflect the light as well). Dry skin can also look lacklustre.
How to fix it?
We need to exfoliate dead dull skin cells. Using a gentle exfoliant such as lactic acid, or glycolic acid if no sensitivity and this can give immediate improvements in the look of dry dull menopausal skin. Retinoids also are an essential part of treating
perimenopausal skin. They increase cell turnover revealing a brighter radiant complexion.
Acne
One of the most frustrating effects for women of menopausal skin is acne. They feel that this should be left in their teenage years. But unfortunately for some it can be quite severe, despite dry skin. How to fix it?
A salicylic acid face wash can help clear pores alongside a retinoid - ideally prescription as the gold standard in acne treatment. Other treatment options that can help
We discussed above the significant decrease in collagen during those first five years post menopause. In clinic an innovative way to combat this is collagen induction therapy. One such example of this is micro needling in which a device stamps thin needles into numbed skin. This stimulates wound healing and creates new micro channels in the dermis. This process induces the formation of new collagen.
Another example is radiofrequency microneedling which induces longer term dermal remodelling by creating micro injuries at the level of the dermis, setting off the wound healing cascade. Insulated needles release radiofrequency currents upon reaching the dermis, creating thermal zones which trigger neo elastogenesis and neocollagenesis. The depth of the needle can be adjusted accordingly to target different layers of the dermis. Radiofrequency microneedling is considered superior to microneedling alone, as it reaches a deeper layer of the skin and has less downtime.
Hormonal acne, menopausal skin and stretch marks are just a few of the many dermatological issues that healthcare professionals encounter in the community. Long waiting lists for tertiary care and the classification of the vast majority of these conditions as non-urgent can result in many patients suffering for years with symptoms that could be easily alleviated with the right treatment plan. The advent of more specialised, focused primary care and continuous reeducation about the treatment modalities for these common presentations is crucial for ensuring an optimal patient experience. By factoring in the latest clinical guidelines and tailoring our approach to fit each unique presentation, we can not only ensure that our patients are visibly healthier, but that they reap the vast psychosocial benefits that come with clear, healthy skin.
PHARMACYNEWSIRELAND.COM 62
Menopause
Acne &
NEW
Rescue Day Gummies Orange Flavour
Bach Rescue Gummies are soft, chewy and tasty orange flavoured gummies containing our natural Bach RESCUE Flower Essences which help you get the most out of your busy day.


• 5 Bach Original Flower Essences

• Vegan (plant-based and gelatine-free)
• No artifiical flavours, colours, preservatives or sweeteners
Ingredients: Glucose syrup, sugar, gelling agent (pectin), acid (citric acid), concentrates of paprika and carrot, natural orange flavouring with other natural flavourings, medium chain triglycerides (from coconut and rapeseed oil), glazing agent (carnaubba wax), flower essences (Helianthemum nummularium, Clematis vitalba, Impatiens glandulifera, Prunus cerasifera, Ornithogalum umbellatum (RESCUE))
Rescue Night Gummies Raspberry Flavour


Bach RESCUE NIGHT Gummies are easy-to-take at bedtime to help prepare for a restful night’s sleep. These tasty, raspberry flavoured gummies are made with our natural Bach RESCUE Flower Essences blend, plus White Chestnut essense to help switch off the mind from unwanted, repetitive thoughts.
• 6 Bach Original Flower Essences
• Vegan (plant-based and gelatine-free)
• No artificial flavours, colours, preservatives or sweeteners
Ingredients: Glucose syrup, sugar, gelling agent (pectin), acid (citric acid), concentrates of carrot and cherry, natural raspberry flavouring with other natural flavourings, medium chain triglycerides (from coconut and rapeseed oil), glazing agent (carnauba wax), flower essences (Aesculus hippocastanum, Helianthemum nummularium, Clematis vitalbba, Impatiens glandulifera, Prunus cerasifera, Ornithogalum umbellatum (RESCUE NIGHT))
Available to order from Wholefoods. Please contact 01 6262315 or your local sales representative.




Ireland’s No. 1 Provider of Ostomy Products & Services Contact our Ostomy Care team for further information Telephone: 01 463 2300 Customer Care Over 20,000 calls handled annually from our customer care team. Complimentary Cutting Service Cutting up to 10,000 bags per week. Training Partnership Ostomy Excellence – we provide a complimentary education programme. Complimentary wipes and bags For Pharmacists to offer their patients. Expanding Range We continue to expand our range as Ireland’s leading stockist for Ostomy & Urology products.
Aspiring to Cervical Cancer Elimination
On November 17th, 2020, the World Health Organization announced its strategy for the worldwide elimination of cervical cancer. It called on all countries to commit to developing realistic and achievable action plans with this aim by the year 2030. Dr Tedros Adhanom Ghebreyesus, the Director-General of the WHO in 2020, stated:
world had permanently eradicated a disease, so that there are zero infections from that organism, is smallpox.
On November 17th, 2020, the World Health Organization announced its strategy for the worldwide elimination of cervical cancer. It called on all countries to commit to developing realistic and achievable action plans with this aim by the year 2030. Dr Tedros Adhanom Ghebreyesus, the DirectorGeneral of the WHO in 2020, stated:
How will elimination be achieved?
"Through cost-effective, evidence-based interventions, including human papillomavirus vaccination, screening and treatment of precancerous lesions, and improving access to diagnosis and treatment of invasive cancers, we can eliminate cervical cancer as a public health problem and make it a disease of the past."
“Through cost-effective, evidence-based interventions, including human papillomavirus vaccination, screening and treatment of precancerous lesions, and improving access to diagnosis and treatment of invasive cancers, we can eliminate cervical cancer as a public health problem and make it a disease of the past.”
This is an incredible step forward for women’s health and we know that it is achievable. Challenges exist in lower- and middle-income countries, where the burden of this disease is greatest. Ireland is on track to be among the first countries worldwide to make cervical cancer a rare disease. Collaboration and partnership between all professionals in the healthcare community will help to make this goal a reality.
What does Elimination of Cervical Cancer mean?
As a result of the enormous advances that have been made in research around human papillomavirus (HPV) and its connection to cervical cancer, we are in the remarkable position of being able to identify a causative factor for over 92% of cervical cancers and, through the widespread use of vaccination in the appropriate age groups, work towards a world where HPV is no longer prevalent in our communities. The WHO target states that if 90% of girls are vaccinated by the age of 15, and 70% of people with a cervix have at least 2 well-timed screening tests while 90% of those diagnosed with pre-cancer or invasive cancer have appropriate treatment and management, then the disease will become extremely rare.
Written by Dr Sarah Fitzgibbon, Primary Care Clinical Advisor, CervicalCheck

This is an incredible step forward for women’s health and we know that it is achievable. Challenges exist in lower- and middle-income countries, where the burden of this disease is greatest. Ireland is on track to be among the first countries worldwide to make cervical cancer a rare disease. Collaboration and partnership between all professionals in the healthcare community will help to make this goal a reality.
It is important to realise that elimination of a disease is not the same as eradication. The WHO states that elimination of cervical cancer is achieved by a country when fewer than 4 cases of cervical cancer are diagnosed for every 100,000 women in its population. This means that the number of women and people with a cervix who are diagnosed with cervical cancer is reduced to a very low number. It is important to understand that it does not mean that there will be no cases Importantly, when a disease is eliminated, prevention measures need to continue to maintain the low rates of disease.
Global Inequities in Cervical Cancer
countries are not attributable to differences in cervical infection with oncogenic HPV types. Instead, they are mainly attributable to the relative lack of high-quality cervical cancer screening and lack of widespread high-quality treatment of invasive cervical cancer in those countries. The proportion of women with cervical cancer who die from the disease is greater than 60% in many low- and middleincome countries, which is more than twice the proportion in many high-income countries, where it is as low as 30%.
Cervical Cancer in Ireland –where are we now?
What does Elimination of Cervical Cancer mean?

Eradication means no cases at all and is only possible when there is a single cause of a condition, and it is possible to permanently remove that cause. An example of where the world had permanently eradicated a disease, so that there are zero infections from that organism, is smallpox.
How will elimination be achieved?
Few diseases reflect global inequities as much as cancer of the cervix. Approximately 90% of the worldwide death from cervical cancer in 2019 occurred in low- and middle-income countries.
The burden of cervical cancer is greatest in these countries because access to public health services is limited, and screening and treatment for the disease have not been widely implemented.
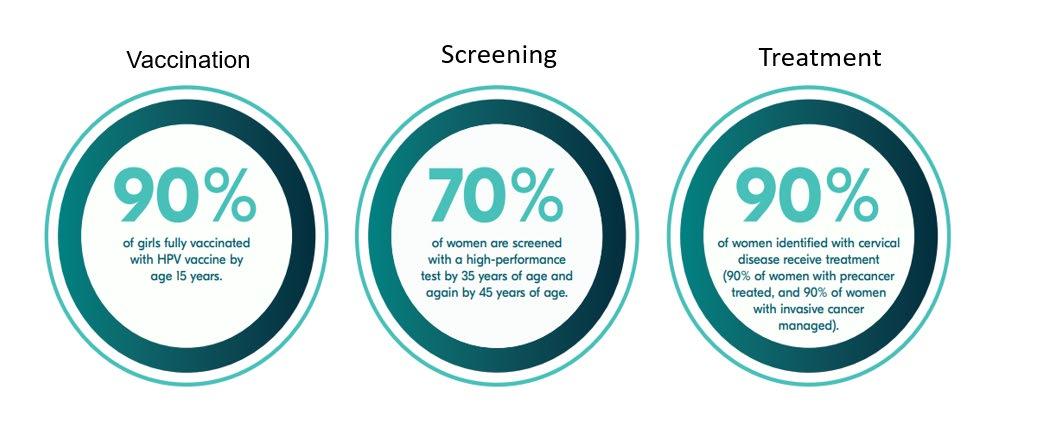

As a result of the enormous advances that have been made in research around human papillomavirus (HPV) and its connection to cervical cancer, we are in the remarkable position of being able to identify a causative factor for over 92% of cervical cancers and, through the widespread use of vaccination in the appropriate age groups, work towards a world where HPV is no longer prevalent in our communities. The WHO target states that if 90% of girls are vaccinated by the age of 15, and 70% of people with a cervix have at least 2 well-timed screening tests while 90% of those diagnosed with precancer or invasive cancer have appropriate treatment and management, then the disease will become extremely rare.
It is important to realise that elimination of a disease is not the same as eradication. The WHO states that elimination of cervical cancer is achieved by a country when fewer than 4 cases of cervical cancer are diagnosed for every 100,000 women in its population. This means that the number of women and people with a cervix who are diagnosed with cervical cancer is reduced to a very low number. It is important to understand that it does not mean that there will be no cases. Importantly, when a disease is eliminated, prevention measures need to continue to maintain the low rates of disease. Eradication means no cases at all and is only possible when there is a single cause of a condition, and it is possible to permanently remove that cause. An example of where the
Cervical cancer diagnosis often occurs when women are in the prime of their lives, undermining their personal wellbeing and livelihood. This has significant impact on the women themselves, but also on their families, communities, and society in general. The loss of a young mother, worker, community member and/or care provider has massive ripple effects in the wider community.
The higher rates of cervical cancer incidence and mortality in low- and middle-income
The current incidence rate of cervical cancer in Ireland is 10.7 per 100,000, as per the most recent available data from the NCRI. We have seen significant improvement on this over the past 14 years, since the introduction of a national cervical screening programme, with a 2.8% decrease year-on-year since 2009. This is a very positive trajectory in our journey towards elimination, but we need to increase our efforts in order to ensure that we achieve the goal of an incidence rate of fewer than 4 per 100,000. While our main weapon in this fight will be HPV vaccination, we know that 40% of people who are diagnosed with cervical cancer in Ireland each year have never been screened, and it is this population of women who would benefit most from our screening efforts.
Vaccination
The uptake rate for the first dose of the HPV vaccine in the 2020/2021 academic year was 80%, with 77% of students having received the second dose in that academic year.
The National Immunisation Advisory Committee has recently changed their advice about the number of HPV vaccine doses needed because of the emergence of new evidence. This shows that in people aged up to 25 years old with healthy immune systems, there is no major difference in the effectiveness of the vaccine between people who get one, two or three doses of HPV vaccine. This is great news because it means fewer injections for our young people and greater availability of the vaccine. People who are immunocompromised will still require three doses.
PHARMACYNEWSIRELAND.COM | 65
Global Inequities in Cervical Cancer
of cervical cancer may include: vaginal spotting or unusual discharge, pain during sex, pain in the pelvis).
3. Promote the HPV vaccination programme
4. Encourage any individual with a symptom to make an appointment with their GP
5. Display leaflets and posters within their pharmacies about risk reduction and screening for cervical cancer
6. Smoking cessation is an important aspect of risk reduction when it comes to cervical cancer
7. Support other healthcare professionals to understand the importance of cervical screening, recognising symptoms and understanding how to discuss these topics with patients
What is the Pharmacist’s role in cervical cancer prevention and elimination?
Vaccination
The uptake rate for the first dose of the HPV vaccine in the 2020/2021 academic year was 80%, with 77% of students having received the second dose in that academic year.
may ask for advice regarding symptoms which are related to cervical cancer, such as unusual vaginal discharge or bleeding, and the pharmacist is well placed to direct that person towards their GP for further investigation.
8. Be a source of ongoing support for patients with cervical cancer
9. Stay up to date on information about risk reduction, screening, and early diagnosis of cervical cancer
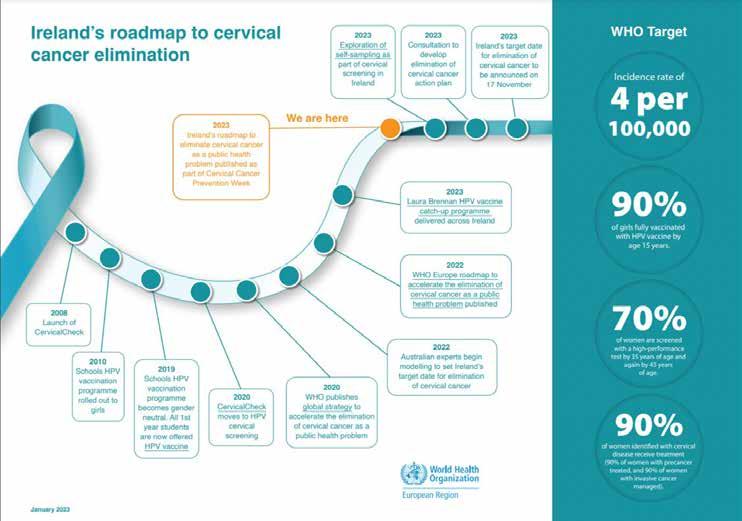
As in integral part of the primary healthcare community, we know that pharmacists play a crucial role in supporting people to make healthy decisions and can encourage healthseeking behaviours. People will turn to their trusted pharmacist for information, and the pharmacy will often be their first port of call for professional medical advice. Pharmacists meet people both when they are well and unwell and so can use multiple opportunities for promoting preventative health.
The National Immunisation Advisory Committee has recently changed their advice about the number of HPV vaccine doses needed because of the emergence of new evidence. This shows that in people aged up to 25 years old with healthy immune systems, there is no major difference in the effectiveness of the vaccine between people who get one, two or three doses of HPV vaccine. This is great news because it means fewer injections for our young people and greater availability of the vaccine. People who are immunocompromised will still require three doses.
Pharmacists could:
What is the Pharmacist’s role in cervical cancer prevention and elimination?
As in integral part of the primary healthcare community, we know that pharmacists play a crucial role in supporting people to make healthy decisions and can encourage health-seeking behaviours. People will turn to their trusted pharmacist for information, and the pharmacy will often be their first port of call for professional medical advice. Pharmacists meet people both when they are well and unwell and so can use multiple opportunities for promoting preventative health
Pharmacy teams are vital to improving the public’s health and are a prominent social and health asset within all communities. Community pharmacy teams have a pivotal role to play in improving people’s health and helping to reduce health inequalities.
Pharmacy teams are vital to improving the public’s health and are a prominent social and health asset within all communities Community pharmacy teams have a pivotal role to play in improving people’s health and helping to reduce health inequalities.
The specific areas where pharmacists can support Ireland’s trajectory towards cervical cancer elimination are through raising awareness of the benefits of HPV vaccination, promoting screening participation, and supporting overall healthy behaviours. People
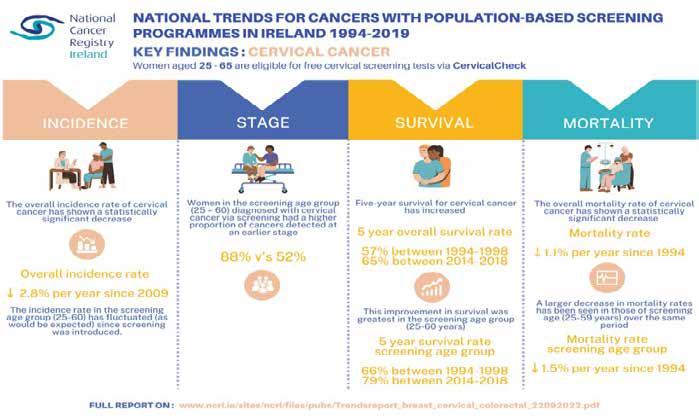
1. Encourage patients to take up their screening appointment - explaining the importance to patients and dispelling any myths about the purpose of the test. (A cervical screening test is a free test to check the health of the cervix. The cervix is the opening to the womb from the vagina. It’s not a test for cancer, it’s a test to see if the person is at risk of developing cancer. If someone has a cervix, they can get cervical cancer. 9 in 10 cervical cancers are caused by certain types of human papillomavirus (HPV). HPV is spread through any kind of sexual contact with a man or a woman)
The specific areas where pharmacists can support Ireland’s trajectory towards cervical cancer elimination are through raising awareness of the benefits of HPV vaccination, promoting screening participation, and supporting overall healthy behaviours. People may ask for advice regarding symptoms which are related to cervical cancer, such as unusual vaginal discharge or bleeding, and the pharmacist is well placed to direct that person towards their GP for further investigation.
Pharmacists could:
2. Educate the public about cervical cancer – including symptom awareness (Cervical cancer symptoms are not always obvious. Unusual bleeding from the vagina is usually the first noticeable symptom of cervical cancer. This includes bleeding: outside of normal periods, during or after sex, after the menopause. Other symptoms
10. Be an advocate and come to us with common concerns or information needs you see in your community.
Pathway to Elimination
By the end of 2023, we will be in a position to predict the date by which Ireland can eliminate cervical cancer. This is a ground-breaking step forward for everyone involved in healthcare in Ireland. By working together to raise awareness of cancer symptoms and promote HPV vaccination and cervical screening, it is possible to reach a point where cervical cancer will be a rare disease in Ireland.
Where can I learn more?
• National Screening Service - Cervical cancer elimination
https://www.screeningservice.ie/cervicalcancer-elimination.html
• To find out more about HPV vaccination in Ireland, including information about the Laura Brennan HPV vaccination campaign which is offering vaccination to women up to the age of 25, go to www.hpv.ie
• There is also more information here about how vaccination to prevent cancer: https:// www.youtube.com/watch?v=aeY8B7jQ2WE
• The Irish Cancer Prevention Network has published a number of webinars on the various ways people can reduce their risk of cancer: https://www.youtube.com/@ nationalcancercontrolprogr5166/videos
• Find out more about smoking cessation initiatives from Tobacco Free Ireland here: https://www.youtube.com/ watch?v=qE4R2E8q9r4
Together we can make cervical cancer a rare disease
Through the global efforts of researchers, public health experts, clinicians and allied health professionals, the aspiration of cervical cancer elimination has become possible. Pharmacists will play a central role in supporting the public to participate in the preventative measures that will make this goal a reality.
66 | PHARMACYNEWSIRELAND.COM
Where can I learn more? • National Screening Service - Cervical cancer elimination https://www.screeningservice.ie/cervical elimination.html



= than sanitary pads 4x drier Result of product demonstration consisting of pouring 4x 10 ml liquid to 1 Always Unnoticeable Protection for Incontinence Normal & 1 Al ways Ultra Long pad. 20 minutes from finishing last pour, plotting paper pressed on both pads, resulting in measuring the level of dryness. for SENSITIVE BLADDER www.prl.ie pgsales@prl.ie +353 1 257 4650 PRL SALES ULC, Greenogue Business Park, Rathcoole, Co. Dublin Logistics Solutions In-Market Solutions Integrated Services
Do You Know How Nutrition Can Impact Fertility?
Traditionally the main focus of nutrition and fertility has been on weight management, restoring ovulation function, and lifestyle factors such as quitting smoking and reducing alcohol intake. While the positive impact of these changes has been documented, there is emerging evidence to suggest that specific dietary strategies can optimise egg and sperm quality. Nutrition can also influence health conditions in females that affect fertility. As one in six heterosexual couples in Ireland may experience infertility,1 it is essential that health professionals are aware of how nutrition can impact fertility. It is also important that they understand the Fertility Dietitian’s role in assessing and managing nutrition and lifestyle factors that affect fertility.
Written by Jemma Henry, CORU Registered Dietitian, MINDI, Certified Fertility and Prenatal Dietitian, Post Graduate Diploma in Nutrition and Dietetics, BSC Biochemistry and Molecular Biology and Diploma in Food Science

jemmahenry@nourishmyfertility.ie

Age, health conditions, mechanical issues e.g. blocked tubes, smoking, diet, obesity, and endocrine disruptors are all factors that can affect female fertility. By identifying the modifiable factors that can be influenced by nutrition and lifestyle changes, the impact of these factors can be modulated to optimise fertility.
The key objectives that a Fertility Dietitian will focus on to support a woman’s fertility are optimising egg health, restoring ovulation, reducing inflammation, reducing oxidative stress, managing existing health conditions and improving the overall nutritional adequacy to support fertility and potential pregnancy. Knowing which objective is a priority and which dietary strategies to use are key considerations for the Fertility Dietitian. Optimising egg health is particularly important as age is a major factor affecting female fertility.2 As a woman ages, an increased percentage of eggs contain genetic abnormalities and older eggs are likely to accumulate more DNA errors.3 Oxidative stress — an imbalance between reactive oxygen species (ROS) and protective antioxidants — is associated with reduced oocyte and embryo quality.4,5
As males are found to be solely responsible for 20–30 percent of infertility cases and contribute to 50 percent of cases overall, it is vital that they are considered when advising nutrition and lifestyle changes.6 An accumulation of evidence shows that oxidative stress also plays a role in male
infertility. The sperm membranes contain a large amount of long-chain polyunsaturated fatty acids, making them highly susceptible to oxidation.7 This can lead to an increased risk of DNA fragmentation and further impairments to sperm quality.8 Diet and lifestyle strategies to reduce oxidative stress are also important factors for the Fertility Dietitian to consider when aiming to optimise sperm health.
Nutritional Factors
Nutritional considerations when reducing oxidative stress include increasing antioxidants and anti-inflammatory omega-3 fatty acids to counteract the adverse effects of oxidative stress. The question continues to arise whether there is an actual fertility diet. Currently, there is not enough evidence to determine an official ‘fertility diet’. Literature suggests that there are certain dietary patterns or strategies that can optimise fertility.9,10 These dietary patterns are associated with a Mediterranean-style diet which has been characterised by a high consumption of wholegrains, vegetables (including pulses), fruits, unrefined carbohydrates, olive oil, oily fish and with a low consumption of red meat.9 This diet pattern is in stark contrast to the western diet which is characterised by saturated fat, refined carbohydrates, processed meat and low levels of vitamins and minerals.9 The western diet is considered to be pro-inflammatory as it is associated with higher levels of inflammation which has
been proposed to be related to poor fertility outcomes in both men and women.10 The dietary principles that are associated with the Mediterranean diet have also demonstrated associations with a lower risk of ovulatory fertility and a reduced risk of infertility.11 Studies have shown positive associations between the Mediterranean diet and improvements in Assisted Reproductive Technology (ART) outcomes such as higher embryo yield and the increased probability of achieving pregnancy.12,13 Other diets have been investigated for improvements in fertility in the context of ART and unsurprisingly they share similar dietary patterns to the Mediterranean diet such as emphasising fruit, vegetables, wholegrains, fish and polyunsaturated fatty acids (PUFA) while limiting processed foods.14,15 Although the effect of dietary patterns on pregnancy outcomes in people using ART is still inconclusive, these studies show promise as potential strategies to improve ART-assisted outcomes.16 Healthy eating patterns have also demonstrated a beneficial effect on sperm parameters.17
The Fertility Dietitian will help individuals choose carbohydrates based on their food preferences while considering the glycaemic index (GI) and glycaemic load (GL) of the carbohydrates. The GI is the relative ranking of carbohydrates based on how a carbohydrate affects blood sugar. Carbohydrates that have a low GI rating will have less of an impact on blood sugar than those with a high GI rating. The Glycaemic load
(GL) is a more accurate way to assess the effect of diet on blood glucose concentration because it accounts for carbohydrate quality through the GI and carbohydrate quantity through portion size.18 Studies have shown, that a higher dietary GL was associated with an increased risk of infertility due to anovulation and reduced fecundity (the ability to produce offspring) in women.18,19 The impact of high glycaemic foods has been also shown to impact sperm quality.20
The type of protein appears to be important regarding ovulatory infertility as Chavarro et al found that replacing animal protein with vegetable protein reduced the risk of infertility due to anovulation.21
Another nutritional consideration that the Fertility Dietitian will include in their nutritional assessment is ensuring that the client is receiving 400 µg of folic acid to prevent neural tube defects (NTDs).22 This dosage can be higher if they have been medically assessed to have increased requirements, for example, previous NTDs, malabsorption disorders, or obesity. Interestingly, there is growing evidence that folic acid could also improve other reproductive outcomes including promoting oocyte quality.23
Vitamin D is thought to play an important role in fertility as receptors are found in the ovaries, endometrium, placenta, pituitary gland, and sperm and testicles.24 Observational studies show that vitamin D deficiency is a risk marker for reduced fertility but is still not clear whether vitamin D supplement improves fertility.25 In the case of vitamin D deficiency during infertility treatment, vitamin D supplementation may benefit women with disorders like polycystic ovary syndrome, insulin resistance, or low antimullerian hormone levels.26 Vitamin D deficiency and insufficiency are also associated with poorer
PHARMACYNEWSIRELAND.COM 68 Fertility
OVULATION TRACKER
WE’RE READY WHEN YOU ARE
Introducing the latest in fertility care: Medicare femSense ® Ovulation Tracker is

CONFIRMS OVULATION SKIN FRIENDLY 7 DAY MEASUREMENT
The Temperature Method
Your basal body temperature is your temperature when you are fully at rest. During ovulation, the increased levels of progesterone result in a minute rise in your basal body temperature. This tiny rise in temperature can be very difficult to spot but can be used as a reliable indication that ovulation has taken place.
For years, women have been using the ‘temperature’ method when trying to conceive but in recent times it has become inconvenient and time-consuming with conventional basal thermometers. Medicare femSense® takes the hassle out of the process by giving continuous measurements, collecting and interpreting the data over a 7-day time period measuring and confirming ovulation. The technology behind Medicare femSense® catapults the temperature method into the 21st century.

Easy to Use
The smart sensor patch is worn for a maximum of seven days – during the fertile window. This is detected based on when the last period was entered in the app. As soon as the patch is applied and activated, the 24/7 measurement begins. The disposable temperature patch is worn under the arm 24/7 for a period of up to 7 days when a woman is most fertile, during this time it continuously measures, records and analyses body temperature data. This data is then transferred from the patch to the phone when scanned using NFC (contactless).
Precise measurement and an intelligent algorithm mean that Medicare femSense® can detect the tiny increase in body temperature caused by ovulation. The patch can then inform the user, via the app, that ovulation has been detected and the patch can be removed.

an innovative 24/7 temperature patch that detects your fertile window to measure and confirm ovulation.
Available exclusively through Fleming Medical. See FLEMINGMEDICAL.IE/FEMSENSE for more information.
Contact your local Fleming Medical representative to learn more, Freephone 1800 307777.
ART outcomes in women.27
Currently, there is no specific recommendation for Vitamin D in Ireland for women trying to conceive. The EFSA has very recently updated its guidance to advise that 12-65-year-olds should supplement 15 µg (600 IU) of Vitamin D for the winter months or daily if individuals are of darkerskinned ethnicity or pregnant.67 Other authors have suggested higher levels of Vitamin D for those trying to conceive.25
Dietary strategies will also focus on increasing foods that contain nutrients such as Zinc, Iron, and B12. Zinc is involved in spermatogenesis, ovulation, and oocyte maturation while iron deficiency is associated with ovulatory infertility.28-30 Vitamin B12 deficiency individually and in combination with hyperhomocysteinemia is associated with early pregnancy loss.31
In practice, the Fertility Dietitian will encourage monounsaturated and polyunsaturated fats while reducing trans and saturated fat. The rationale for this is based on observational studies that have shown a higher amount of trans fats is associated with a higher risk of ovulatory infertility and reduced fecundability.32-33 Omega 3 fatty acids are essential fatty acids, that have a significant antiinflammatory effect.34 These have been associated with a higher probability of clinical pregnancy and live birth in women undergoing infertility treatment with ART.35 Most recently a systematic review summarised the emerging association between omega-3 intake through diet and favourable IVF/ICSI outcomes, possibly via its effect on egg quality.36
Caffeine and alcohol are also other important factors to consider as part of the nutritional assessment. The European Food Safety Authority guidelines advise women who are trying to conceive or are pregnant to keep caffeine intake below 200 mg to reduce negative pregnancy outcomes.37 While increased caffeine consumption is associated with spontaneous abortion and (>500mg per day) may affect time to pregnancy, there is a lack of evidence to show that there is an association between caffeine and fecundity or caffeine and IVF/ICSI outcomes.38-41 The HSE advises women who are trying to conceive to aim to avoid alcohol but to what extent alcohol consumption affects female fertility remains unclear.42 Female alcohol consumption is associated with reduced fecundability and another study also suggested that modest drinking levels may decrease fecundability if consumed during critical physiologic intervals of the menstrual cycle.43,44 Drinking more than 84g of alcohol per week (1 alcoholic beverage=12g of alcohol) was associated with reduced IVF/ ICSI outcomes in both men and women.41 While there are studies showing how alcohol affects sperm quality in heavy drinkers there is little evidence to demonstrate alcohol’s effect on fecundability in the male.45,46
As well as looking at lifestyle factors such as smoking, reducing exposure to endocrine disruptors
is also a significant part of the advice given by the Fertility Dietitian. Endocrine Disrupting Chemicals (EDCs) are ubiquitous exogenous substances that can mimic or interfere with the endocrine system. Examples of EDCs include bisphenol A, phthalates, pesticides, and pollutants such as dioxin and polychlorinated biphenyls (endocrine society) The main way humans are exposed to them is through diet. EDCs can affect conception, in-utero development, neonatal life, and long-term child and maternal health by affecting both male and female reproductive processes. Complete avoidance is impossible, but dietary alterations such as avoiding plastic bottles and packaging have been shown to reduce exposure.47
Health conditions impacted by nutrition

In support of how important nutrition’s role is in managing female infertility, Kumar et al have proposed a self-administered screening tool to identify women that would benefit from nutritional intervention to improve fertility. This screening tool is awaiting validation. This publication also summarises health conditions such as Polycystic ovary syndrome (PCOS), Endometriosis and being over/underweight as health conditions that can be nutritionally optimised to improve female fertility.48
PCOS is the most common endocrine disorder in women of
reproductive age. It is the leading cause of anovulatory infertility.49 The key role of dietary intervention with PCOS is to restore ovulation, restore menstrual cycle regularity, reduce insulin resistance and reduce weight if necessary. While lifestyle management is recommended as first-line treatment of PCOS, the optimal dietary composition is unclear.50 Focusing on low GI food is one of the approaches the Fertility Dietitian will use to reduce insulin resistance and restore menstrual regularity.51 As there is a high prevalence of women in this PCOS population that are obese or overweight, research suggests that approximately 5 percent of weight reduction is adequate to improve insulin resistance, high levels of androgens, reproductive system dysfunctions, and fertility in overweight women with PCOS.50 Endometriosis is an oestrogendependent, chronic inflammatory disease affecting up to 10 percent of women of reproductive age.52,53 It is also a systemic condition and has been found on virtually all organs.54 Some women with Endometriosis are asymptomatic, while for others, it is a debilitating condition that can cause pain and infertility.55 The pathophysiology of infertility in mild cases of Endometriosis is not understood but it has been associated with anatomical disturbances in severe cases.54 It has also been linked to a negative impact on egg quality.53 As Endometriosis is an inflammatory condition, dietary approaches often include focusing on foods with anti-inflammatory properties such as omega 3 fatty acids and antioxidants from fruit and vegetables, herbs/spices that contain polyphenols/ flavonoids and reducing processed food.56 While the research suggests that increased consumption of omega-3 has a positive effect on Endometriosis the overall evidence for using an an-inflammatory approach remains unclear.57 Higher amounts of red meat, alcohol and trans fats are associated with an increased risk of Endometriosis.58-60 Part of the Fertility Dietitian’s role in this area of Endometriosis is symptom management. Visceral hypersensitivity is a key feature in both Irritable Bowel Syndrome (IBS) and Endometriosis and may explain why they share similar symptoms.61 A low FODMAP diet which has been investigated for its effectiveness for individuals with IBS may be an effective dietary strategy for women with gut symptoms and Endometriosis.62,61
A significant association between IBS, Eating Disorders (ED), and Endometriosis was demonstrated in the ENDONUT trial where the prevalence of IBS and ED
PHARMACYNEWSIRELAND.COM 70 Fertility
It’s that simple... ... for all women capable of conceiving.
Folic Acid - helps prevent Spina Bifida and other NTDs1. Clonfolic is the market-leading brand2. Take one tablet daily.
Key Facts
• Studies have shown over 70% of first time NTDs1, such as Spina Bifida can be prevented by taking 0.4mg of folic acid daily.
• Almost 50% of pregnancies are unplanned.
• It’s important to take 0.4 mg of folic acid every day for at least 14 weeks before you become pregnant and continue taking it for at least the first 12 weeks of pregnancy.
You actually need Folic Acid
Clonfolic.ie
Clonfolic is contraindicated in cases of Vitamin B12 deficiency. Caution is advised for patients under therapy for folate-dependent tumours when taking folic acid. Women with pre-existing diabetes, obesity, family history of neural tube defects, or previous pregnancy affected by neural tube defect have an increased risk of having a pregnancy affected by a neural tube defect and higher doses should be considered. For women taking anti-seizure medication the requirement for folic acid may be different and they should be under the supervision of a physician while taking folic acid supplements. The tablet also includes lactose monohydrate. A copy of the summary of product characteristics is available on request. Clonfolic 0.4mg tablets. PA 126/95/1. PA Holder: Clonmel Healthcare Ltd, Waterford Road, Clonmel, Co Tipperary, Ireland. www.clonmel-health.ie Medicinal product not subject to medical prescription. Supply through general sales.
References: 1. NTDs (neural tube defects). 2. Leading sales brand in pharmacy – IQVIA, IRLP audit, units, MAT Jan 20. Date prepared July 2020. 2020/ADV/CLO/048H
Fertility
in women with Endometriosis was higher than in the general population.63 This has further implications for the dietary strategy used by the Fertility Dietitian as they will have to also consider an individual’s relationship with food while achieving nutritional adequacy to support a potential pregnancy. Weight management is also an important consideration for the Fertility Dietitian when trying to optimise fertility. Obesity is a known risk-factor for infertility. It has been shown to affect ovulatory function, time to conception and is associated with poor reproductive outcomes in assisted conception.64,65 However there is insufficient evidence to suggest that short-term weight loss before ART improves outcomes.67 National Clinical Guidelines advise maintaining a BMI of 19-25 kg/m2 as part of recurrent miscarriage management advice.66 Low body weight can also affect fertility by impacting ovulation while increasing body weight may improve the chance of conception.64
Conclusion
Although questions still remain unanswered it is clear that nutrition
and lifestyle play a critical role in impacting both male and female fertility. While we do not have an official fertility diet, there are dietary patterns/ strategies that can positively affect fertility. Highquality intervention studies are warranted to confirm these dietary patterns/ strategies with a view to developing dietary guidelines that go beyond the traditional advice of weight management, alcohol, and smoking.
As there is an abundance of misinformation on this topic on infertility forums, the internet, social media and from non-qualified practitioners, individuals struggling with infertility are trying diets and supplements which may further reduce their chances of conception and add to an already costly ART journey.
As nutrition and lifestyle factors are modifiable, it is vital that they are part of the infertility management treatment plan for both men and women. This nutrition and lifestyle advice should be given as a consultation to allow for a full nutritional assessment. The appropriate dietary patterns/ strategies and their rationale should be explained to the individual. Furthermore, the level of evidence underpinning each
diet strategy discussed should also be explained in an easyto-understand manner. This will allow the individual to make an informed decision about their nutritional and lifestyle choices which may be impacting their fertility. This will undoubtedly reduce the use of alternative diets and non-evidenced-based supplements that are currently being widely used by men and

women experiencing infertility. It is the unique skill set of the Fertility Dietitian that allows them to assess the available evidence and to determine the most appropriate nutritional plan in order to optimise fertility. The Fertility Dietitian is perfectly placed to be an integral part of the multidisciplinary team for infertility management.
References on request
Clinical Practice Guidelines in Obstetrics and Gynaecology
The HSE has launched a new suite of Clinical Practice Guidelines in Obstetrics and Gynaecology, offering upto-date, evidence-based, clinical recommendations for care of women in maternity and gynaecology services, and promote a standardised approach to care across the country.
In what is an ambitious programme of work, the first twelve National Clinical Practice Guidelines cover areas of maternal and gynaecological care as diverse as Post-Menopausal Bleeding, Stillbirth, Vaginal Birth After Caesarean Section, and Post-Partum Haemorrhage, amongst others.
Led by Professor Keelin O’Donoghue, and supported by Ms Nicolai Murphy as programme manager, the National Clinical Practice Guidelines are a programme of work agreed between the HSE’s National Women and Infants Health Programme (NWIHP) and the Institute of Obstetricians and Gynaecologists of the Royal College of Physicians of Ireland.
Each new guideline will be accompanied by a summary document which will support healthcare professionals with an easy reference guide, and a plain language summary which explains the impact the new Guideline will have on women’s care in a simple format.
The Guideline Programme Team is also using a mobile application (app) to facilitate easier access to the guidelines for working healthcare professionals around the country.
The following guidelines have been developed and will be launched today:
1. Assessment and Management of Postmenopausal Bleeding
2. Assessment and Management of Stress Urinary Incontinence in Women
3. Diagnosis and Management of Placenta Accreta Spectrum
4. Diagnosis and Management of Mesh Complications
5. Recurrent Miscarriage
6. Investigation and Management of Complications of Early Termination of Pregnancy
7. Prevention and Management of Primary Postpartum Haemorrhage
8. Diagnosis and Management of Pelvic Organ Prolapse
9. Prevention of early onset Group B Streptococcal disease in term infants
10. Stillbirth - Prevention, Investigation, Management and Care
11. The Fetal Anatomy Ultrasound
12. Vaginal Birth after Caesarean Section
The first suite of guidelines will be followed with over 30 updated Clinical Practice Guidelines during 2023 and 2024.
The updated National Clinical Practice Guidelines can be found at: https://www.hse.ie/eng/about/ who/acute-hospitals-division/ woman-infants/clinical-guidelines/ national-clinical-guidelines.html and
https://www.rcpi.ie/FacultiesInstitutes/Institute-ofObstetricians-and-Gynaecologists/ National-Clinical-Guidelines-inObstetrics-and-Gynaecology
PHARMACYNEWSIRELAND.COM 72
News




Pancreatic Cancer
Pancreatic Cancer: A Public Health Burden
The global incidence and mortality of pancreatic cancer are increasing annually. Worldwide, the incidence is projected to rise to 18.6 per 100,000 by 2050, with the average annual growth of 1.1%, indicating that pancreatic cancer will pose a significant public health burden.
• Ethnicity-more common in African Americans than Caucasians
• Family history
• Blood group A patients have a 40% higher risk than those with other blood types
• Pancreatic microbiota
Presentation and Diagnosis
acholic stools, and dark urine may be present. Patients may present with recent-onset diabetes, and sometimes may present with recurrent deep vein thrombosis (DVT) due to hypercoagulability that prompts clinicians to suspect cancer and a full workup.
“Blood tests include, FBC, U+E, LFTs, coagulation-studies, glucose, and lipid-profile.”
Theresa Lowry Lehnen, Clinical Nurse Practitioner and Associate Lecturer South East Technological University told us more
about the 12th most common cancer worldwide.
Pancreatic cancer is the 11th most common cancer in women, and the 12th most common in men. Theresa notes, “Globally there were more than 495,000 new cases of pancreatic cancer in 2020, and it affects over 600 people in Ireland annually. Despite rapid advances in modern medicine and significant improvements in survival rates of many cancers, pancreatic cancer is still a highly fatal gastrointestinal cancer with difficulty in early detection, and a low 5-year survival rate.
“Pancreatic cancer 5-year survival rates range from 2% to 9%, with little difference between high and low-income, and middle-income countries. The 5-year survival rate varies globally in different regions and countries, but does not exceed 10%. It is predicted that patients with non-operative pancreatic cancer have a lower 5-year survival rate.
“The estimated global, 5-year survival rate for pancreatic cancer is about 5%. Approximately 90% of all cases are among people over 55 years of age, and the incidence rates for both genders increases with age. Surgical resection is the only current option for a cure, however, only 20% of pancreatic cancer is surgically resectable at the time of diagnosis.”
Aetiology and Risk Factors
The aetiology of pancreatic cancer is poorly understood, Theresa says. 95% of tumours carry mutations in the K-RAS2 proto-oncogene, the activation of which leads to increased cell proliferation, loss of the normal response to apoptotic signals, dysplasia and ultimately cancer.
In the pancreas, K-RAS mutations tend to cause the development of precancerous lesions called pancreatic intraepithelial neoplasia (PIN), which are present in up to a third of older people, but will only lead to cancer in about 1% of cases. It is estimated that it takes up to 20 years from the time of the first mutation to develop the fullblown disease.
Many non-modifiable and modifiable risk factors are associated with pancreatic cancer.
• Age older than 55 years
• Smoking
• Diabetes
• Obesity
• Chronic pancreatitis
• Cirrhosis of the liver
• Helicobacter pylori infection
• Work exposure to chemicals in the dry cleaning and metalworking industry
• Gender-more common in males than females
Theresa explains, “Symptoms of pancreatic cancer include; pain or discomfort in the abdomen, which may spread to the back; unexplained weight loss; indigestion; jaundice; loss of appetite; nausea; feeling full very quickly; a lasting change in bowel habits-steatorrhea; a new diagnosis of diabetes without weight gain; and tiredness.
“Sometimes there may be no signs or symptoms in the early stages of pancreatic cancer. Diagnostic tests include, history, examination, laboratory tests, transabdominal ultrasound, abdominal CT scan, PTC (percutaneous transhepatic cholangiography), MRCP scan (magnetic resonance cholangiopancreatography), Endoscopic Ultrasound (EUS), Laparoscopy and Biospy.
“General examination may reveal jaundice, pallor, skin excoriations or weight loss/cachexia. Abdominal examination may reveal epigastric tenderness; an upper abdominal mass; nodular hepatomegaly; ascites; and a palpable gallbladder. Courvoisier’s law states that the presence of a non-tender enlarged gallbladder means that jaundice is unlikely to be due to gallstones, as chronic cholecystitis causes the gallbladder to become shrunken and fibrotic. A palpable gallbladder is, therefore, a worrying sign. There may also be cervical lymphadenopathy.
“Patients with adenocarcinoma of pancreas typically present with painless jaundice (70%) usually due to obstruction of the common bile duct from the pancreatic head tumour. Weight loss occurs in about 90% of patients and abdominal pain in about 75%.
Weakness, pruritus from bile salts in the skin, anorexia, palpable, non-tender, distended gallbladder,
Staging investigations for patients with confirmed pancreatic cancer include:
• Triple-phase “pancreas protocol” CT scan is the gold standard for assessment of pancreatic cancer. By taking images at different times after IV contrast administration, it provides detailed imaging of the tumour itself, its invasion into surrounding tissues, the degree of vascular infiltration and biliary tree dilatation, and presence of lymphatic or liver metastasis. It can be used to accurately predict surgical resectability in up to 90% of cases.
• Bone scan or PET scan can accurately detect distant metastases.
• Diagnostic laparoscopy is used to rule out intraperitoneal spread in high-risk patients.
• Biopsies for histopathology can be obtained percutaneously, endoscopically via EUS/ERCP, or laparoscopically and in some cases through an open procedure. Endoscopic biopsy is considered to be the safest and most appropriate approach.
8 Differential diagnosis includes acute pancreatitis, chronic pancreatitis, cholangitis, cholecystitis, choledochal cyst, peptic ulcer disease, cholangiocarcinoma, and gastric cancer.
Treatment and Management
Treatment for pancreatic cancer includes surgery, chemotherapy and radiotherapy. Theresa continues, “The treatment and management of pancreatic cancer is determined by whether the tumour is resectable or not, but other important factors include the patient’s overall health and
PHARMACYNEWSIRELAND.COM 74
An interview with Theresa LowryLehnen (PhD), CNS, GPN, RNP, South East Technological University
fitness for major surgery and postoperative chemotherapy.
“There are surgical treatments available for both resectable cancers and palliate unresectable disease, and these are supported by the use of adjuvant medical therapies such as chemoradiotherapy and pain control measures. If the pancreatic adenocarcinoma is considered locally advanced it is unresectable, and neoadjuvant treatment with chemotherapy and/or radiation is typically preferred in this situation.
“There is a role for radiation therapy in combination with chemotherapy to treat locally advanced pancreatic cancer. Radiation therapy was originally used to alleviate the pain, but its use is now more widespread to shrink tumours and increase survival.
“Pylorus-preserving pancreaticoduodenectomy
(Modified Whipple): Localised tumours in the head of the pancreas or periampullary region are suitable for pylorus-preserving pancreaticoduodenectomy, more commonly known as the modified Whipple procedure. It involves removal of the head of the pancreas, most of the duodenum, the common bile duct and the gallbladder, with or without extended dissection of additional lymph nodes.
“The traditional Whipple’s procedure also includes removal of the pylorus and antrum of the stomach, which is still occasionally necessary depending on the extent of the tumour. If the portal or superior mesenteric veins are involved, they can also sometimes be resected and reconstructed using vein grafts. Once the above organs have been resected, the functional anatomy of the upper GI tract must be restored so the patient can still digest and absorb food.
“This is done by creating a Roux-en-Y loop from a segment of jejunum, and using end-toside anastamoses to make a pancreaticojejunostomy to drain pancreatic juice into the small bowel; a hepaticojejunostomy to drain bile into the small bowel, and a duodenojejunostomy to restore GI tract continuity. This is normally done via a large abdominal “rooftop” incision, but some centres do it laparoscopically. The Whipple is a high-risk procedure requiring careful pre-operative work-up and intensive post-operative monitoring and management.

“Complications of the Whipple procedure include bleeding, sepsis, bile and pancreatic leakage, anastamotic failure, delayed gastric emptying, and
nutritional problems, and patients often remain in hospital for weeks or months while they recover. Patients require long-term pancreatic enzyme replacement in the form of Creon tablets taken with food. Five-year survival for patients with ductal carcinomas is 10-20%, and 40% for patients with other types of pancreatic cancer.
“Distal Pancreatectomy: Patients with localised tumours in the body or tail of the pancreas are suitable for a distal pancreatectomy. This involves removal of the body and tail of the pancreas as well as the spleen. Distal pancreatectomy is a more straightforward procedure than the Whipple and can be done openly or laparoscopically.
“Complications are less frequent but include bleeding, sepsis, pancreatic leakage and pancreatic endocrine insufficiency resulting in diabetes. As the procedure involves a splenectomy, these patients are also at lifelong risk of potentially fatal overwhelming postsplenectomy infections (OPSI).
“Total pancreatectomy: Rarely, patients with localised tumours in or involving the neck of the pancreas, or diffuse cancers such as intraductal papillary mucinous neoplasm (IPMN) may be offered a total pancreatectomy. Complication rates are similar to a Whipple procedure, but with the added risk of post-splenectomy sepsis, and lifelong insulindependent diabetes, which can be difficult to manage.
“Palliative Surgical Treatments: Patients presenting with obstructive symptoms secondary
to inoperable pancreatic cancer may be offered palliative surgical treatments to help control their symptoms. Biliary obstruction and jaundice is common in advanced disease. It leads to malaise, abdominal pain and severe pruritis, and can also put patients at risk of death from cholangitis, renal failure and severe coagulopathy.
“Management options include biliary stenting, endoscopically via an ERCP, or percutaneously using radiological transhepatic techniques, and biliary bypass surgery with choledochojejunostomy, hepaticojejunostomy or sometimes a palliative ‘Whipple’ procedure. Duodenal obstruction is common and presents with symptoms of gastric outlet obstruction such as epigastric pain and profuse nonbilious vomiting. It can be treated endoscopically with duodenal stenting, or gastric bypass surgery using a gastrojejunostomy or Roux-en-Y bypass.
“Pancreatic duct obstruction can lead to pain and malabsorption. It can be treated with endoscopic pancreatic stenting or sometimes with pancreaticoduodenectomy.”
Theresa adds that pain is a significant problem in patients with pancreatic cancer and is generally managed with opiate analgesia, neuropathic adjuncts and the management of obstructive symptoms. “Medical therapies for exocrine cancers may be used as adjuncts to surgery, or as a primary palliative treatment in advanced disease. Patients with unresectable disease may be
offered palliative chemotherapy. Although most pancreatic tumours are chemoresistant, gemcitabinebased regimes can delay disease progression and improve survival in patients with reasonable performance status.
“Radiotherapy can help with pain control, but does not improve survival. Pancreatic enzyme supplementation with Creon tablets can help with malabsorption and weight loss. Advanced metastatic cancer requires individualised palliative treatment with chemoradiotherapy and symptom control. Unresectable or metastatic functional endocrine tumours except for somatostatinomas can be managed medically with somatostatin analogues, which act to control symptoms by suppressing pancreatic hormone secretion.”
Theresa concludes that, “Despite major scientific and medical advances, mortality rates for pancreatic cancer have not improved much since the 1970s. Pancreatic cancer rates continue to rise, and will cause a major economic burden for all countries and related populations in the next two decades. A global prevention and control strategy for pancreatic cancer must include effective tobacco-control policy, recommendations for healthier lifestyles, increased screening, vaccination programmes, and education to improve public awareness and the need to take precautions.”
PHARMACYNEWSIRELAND.COM 75
Topic Team Training – Dehydration
A community pharmacy environment that fosters teamwork ensured high levels of consumer satisfaction. This series of articles is designed for you to use as guide to assist your team in focusing on meeting ongoing CPD targets and to identify any training needs in order to keep the knowledge and skills of you and your team up to date.
be characterized by extreme versions of the symptoms above as well as:
• lack of sweating
• sunken eyes
• shriveled and dry skin
• low blood pressure
• increased heart rate
• fever
• delirium
• unconsciousness
Risk Factors
and lost electrolytes. The best approach to dehydration treatment depends on age, the severity of dehydration and its cause.
For infants and children who have become dehydrated from diarrhea, vomiting or fever, use an over-the-counter oral rehydration solution. These solutions contain water and salts in specific proportions to replenish both fluids and electrolytes.
The below information, considerations and checklist provides support to enable you to run a team training session and identify opportunities for learning within the topic of Dehydration. Dehydration occurs when more water and fluids leave the body than enter it. Even low levels of dehydration can cause headaches, lethargy, and constipation.The human body is roughly 75 percent water. Without this water, it cannot survive. Water is found inside cells, within blood vessels, and between cells.
A sophisticated water management system keeps our water levels balanced, and our thirst mechanism tells us when we need to increase fluid intake.
Although water is constantly lost throughout the day as we breathe, sweat, urinate, and defecate, we can replenish the water in our body by drinking fluids. The body can also move water around to areas where it is needed most if dehydration begins to occur. Most occurrences of dehydration can be easily reversed by increasing fluid intake, but severe cases of dehydration require immediate medical attention.
Key Facts:
• Around three-quarters of the human body is water.
Consider:
The first symptoms of dehydration
• The causes of dehydration include diarrhea, vomiting, and sweating.
• Individuals more at risk of dehydration include athletes, people at higher altitudes, and older adults.
• Early symptoms of dehydration include dry mouth, lethargy, and dizziness.
The first symptoms of dehydration include thirst, darker urine, and decreased urine production. In fact, urine colour is one of the best indicators of a person’s hydration level – clear urine means someone is well hydrated and darker urine means they are dehydrated.

However, it is important to note that, particularly in older adults, dehydration can occur without thirst. This is why it is important to drink more water when ill, or during hotter weather.
As the condition progresses to moderate dehydration, symptoms include:
• dry mouth
• lethargy
• weakness in muscles
• headache
• dizziness
Severe dehydration (loss of 10-15 percent of the body’s water) may
Although dehydration can happen to anyone, some people are at a greater risk. Those at most risk include:
• People at higher altitudes.
• Athletes, especially those in endurance events, such as marathons, triathlons, and cycling tournaments. Dehydration can undermine performance in sports, as this article explains.
• People with chronic illnesses, such as diabetes, kidney disease, cystic fibrosis, alcoholism, and adrenal gland disorders.
• Infants and children – most commonly due to diarrhea and vomiting.
Dehydration in older adults is also common; sometimes this occurs because they drink less water so that they do not need to get up for the toilet as often. There are also changes in the brain meaning that thirst does not always occur.
Treatment
The only effective treatment for dehydration is to replace lost fluids
Key Points:
Check your pharmacy team are aware and understand the following key points:
The pharmacy team knows to what to advise in older adults drinking less water
Start with about a teaspoon (5 milliliters) every one to five minutes and increase as tolerated. It may be easier to use a syringe for very young children. Older children can be given diluted sports drinks. Use 1 part sports drink to 1 part water. Most adults with mild to moderate dehydration from diarrhea, vomiting or fever can improve their condition by drinking more water or other liquids. Diarrhea may be worsened by full-strength fruit juice and soft drinks.
If you work or exercise outdoors during hot or humid weather, cool water is your best bet. Sports drinks containing electrolytes and a carbohydrate solution also may be helpful.
Actions:
Ensure the team can meet the needs of patients who experience dehydration due to everyday non-medical causes (such as excessive sweating) and those who experience dehydration due to common medical conditions (such as gastroenteritis)
Ensure that I and the team are aware of the treatments for dehydration and appropriate counselling
Do we understand the reasons why some people may be at greater risk of dehydration? What are these?
How to identify severe dehydration
When to refer someone for further investigation
Those at greatest risk of suffering from dehydration
Appropriate treatment and advice
The team knows which groups of customers are likely to be at greatest risk of dehydration
My pharmacy assistants can meet the points in this training checklist.
Are we confident on the appropriate amount of ORS to give in the first 4 hours to children and to adults?
Can we provide good advice on dealing with dehydration?
Train the team to meet all the above considerations
76 | PHARMACYNEWSIRELAND.COM
WHEN WATER ISN’T ENOUGH
O.R.S Hydration Tablets contain a balanced combination of glucose, salts and electrolytes.
The soluble tablets replenish water and salts, helping to maintain a proper fluid balance. Perfect for before, during or after exercise.
Fast, proven, hydration, O.R.S is used by:

People who lose excess fluid
Professional and recreational athletes

Visitors to hot or tropical countries

e. info@pharmed.ie t. +353 (0) 44 939 6188 PLACE YOUR ORDER TODAY, CONTACT YOUR LOCAL PHARMED TERRITORY MANAGER
Proud sponsors of the 2023 Mullingar Half Marathon. Annual half marathon in the heart of the Midlands.
Cancer Inequalities and Deprivation
The National Cancer Registry (NCRI) has published a new report entitled: Cancer inequalities in Ireland by deprivation, 2004-2018. This report measures differences in cancer incidence, five-year survival and stage at presentation between populations living in the most and least deprived areas in Ireland for the diagnosis period 2014-2018. Comparative information is also provided for earlier periods (2004-2008 and 2009-2013).
The report can be found at www.ncri.ie
Key findings include:
• Overall, there was a 7% higher age-standardised incidence for males and a 5% higher incidence for females living in most deprived areas compared to those living in the least deprived areas in 2014-2018
• Overall, there was lower fiveyear cancer survival rates in patients from the most deprived areas compared to those in the least deprived areas. Those in the most deprived areas had a 28% higher mortality risk due to cancer within five years of cancer diagnosis compared to those in the least deprived areas, having adjusted for age, gender, and cancer type.
• Differences in the types of cancers diagnosed in the most and least deprived areas, with a higher incidence of stomach, lung and cervical cancer in people living in most deprived areas, while those living in least deprived areas show a higher incidence of breast, prostate, and melanoma and nonmelanoma skin cancer.
• People living in the most deprived areas had a higher risk of late-stage presentation for breast and prostate cancers than those living in least deprived areas. No disparities in stage of presentation were found for lung or colorectal cancers when comparing the least and most deprived groups.
• Although cancer incidence rates have fallen and survival rates have improved over time across the majority of cancers and for all sectors of society, there is no evidence of any reduction in disparities between those living in the least and the most deprived areas.
A range of potential factors may contribute to such disparities, including differences in general health, exposure to particular risk factors, health-seeking behaviour (influencing early detection), access to healthcare,
Cancer inequalities in Ireland 2004 -2018
Age-standardised cancer incidence: most vs. least deprived
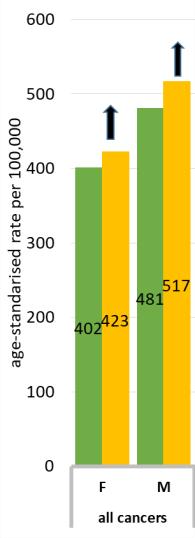
Summary Figure 1.
Age-standardised cancer incidence, Ireland, 2014 -2018: comparison between the most and the least deprived quintiles.
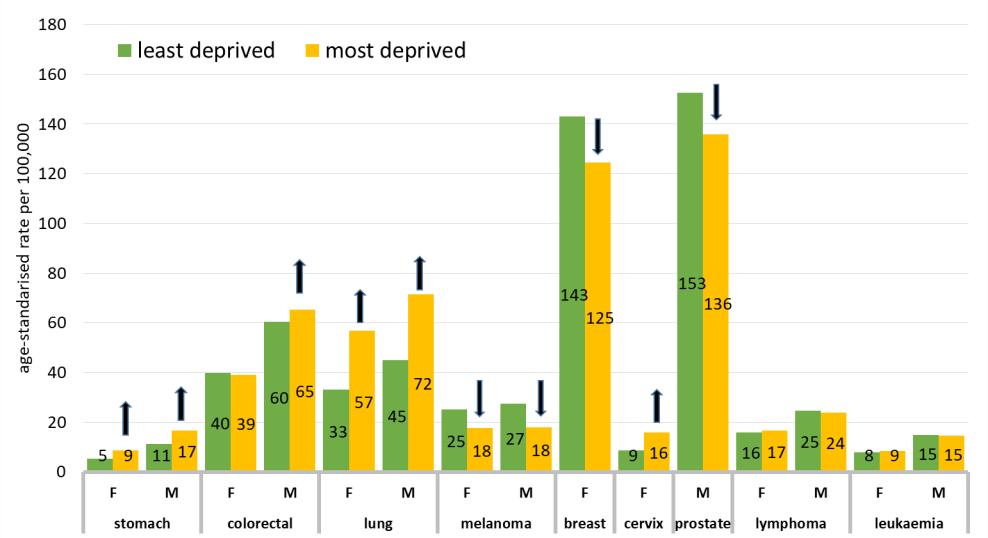
Arrows indicate direction of difference and significance at the 95% confidence level
What was found?
Five-year survival
• The most deprived quintile of the population in 2014-2018 had significantly poorer five-year survival (mortality hazard 28% higher than the least deprived quintile ) for cancer as a whole, with similar findings for the two earlier periods.
• Five-year survival was poorer for the most deprived quintile of the population compared with the least deprived quintile for colorectal, lung, melanoma, breast and prostate cancers for the most recent period 2014-2018 and (with the exception of melanoma) for the two earlier periods.
• There was no significant narrowing or widening of survival disparities over time.
• This data is summarised in Figure 2.
or other factors that may be linked to socioeconomic or geographic factors. Disentangling these factors and their relative importance is far from straightforward, and many challenges remain in tackling the root causes of such inequalities.
Chair of the NCRI Board Dr Jerome Coffey, welcomed the report and said, “These important data underline the known links between socioeconomic deprivation and cancer incidence and survival, with no major reductions in disparities
between groups over the time periods examined. Prevention, screening and early diagnosis are major elements of the National Cancer Strategy 2017-2026 and will have to remain as priorities in subsequent strategies.”
NCRI co-author Dr Niamh Bambury said, “There is an increased focus on cancer inequalities experienced across the cancer continuum as part of Europe’s Beating Cancer Plan. Monitoring cancer inequalities is important to identify groups who might benefit from targeted
risk reduction interventions and to assess the impact of cancer strategies. This report provides the most up-to-date, reliable information on the effect of deprivation on cancer incidence and five-year survival. The socioeconomic and individual factors that contribute to cancer disparities are manifold and require a whole system response. In the health field, advancement of policy initiatives, including Sláintecare and Healthy Ireland, are needed to help address the root causes of these disparities.”
PHARMACYNEWSIRELAND.COM 78 Report
8
New Partnership for Allcare Pharmacy


RTÉ Media Sales has announced Allcare Pharmacy as the new sponsor of Today with Claire Byrne, RTÉ Radio 1, Monday – Friday, 10am-12pm.
Brokered by Javelin, the 11-month RTÉ Radio 1 sponsorship includes 6 x 10-second sponsor-credited stings per show, sponsor-credited promos in Rising Time, Liveline, Drivetime, Saturday with Colm O’ Mongain and Brendan O’ Connor as well as podcast and homepage sponsorship.
Today with Claire Byrne is currently joint seventh most listened-to radio programme in the country, with a daily audience of 344,000.
Caroline Burton, Head of Retail Marketing at Uniphar Group said “Allcare Pharmacy is delighted to partner with Claire Byrne and RTE Radio 1 in 2023. As Ireland’s largest community pharmacy network, it was important for us to find a partner which reflects the informative, entertaining and important topics of the day that matter to our customers. Today with Claire Byrne is a perfect fit
for a trusted community pharmacy brand like Allcare Pharmacy.”

Geraldine O’Leary, Commercial Director, RTÉ said: “RTÉ Media Sales are delighted to welcome Allcare Pharmacy as our new sponsor of Today with Claire Byrne. Allcare Pharmacy is a valued partner, and we look forward to working with them across this exciting opportunity.
Aoife Hofler, Director, Javelin, said: “We are delighted to go live this week with the full broadcast sponsorship of Claire Byrne on RTÉ Radio 1. Our strategy for Allcare Pharmacy is to bring the brand front of mind for a broad audience, with high frequency to continuously remind and prompt consumers to visit their local Allcare pharmacy. Being the seventh most listened to Irish radio show, Claire Byrne allows us to do this effectively with mass weekly reach and high frequency.”

PHARMACYNEWSIRELAND.COM 79 News
Pictured Left to right are Caroline Burton, Head of Retail Marketing at Uniphar Group, Geraldine O’Leary, Commercial Director, RTÉ, and Aoife Hofler, Director, Javelin.
CROSS BORDER NETWORK LAUNCHES TO BRING HOPE TO FAMILIES AFFECTED BY RARE DISEASES
University College Dublin (UCD), Queen’s University Belfast, and 33 partners have launched the All-Ireland Rare Disease Interdisciplinary Research Network (RAiN).
Individual rare diseases may be rare but collectively impact more than 400,000 people across the island of Ireland. There are as many people living with rare diseases across Ireland as live with diabetes, yet rare diseases receive much less recognition and support.
Many people living with a rare disease experience chronic debilitating illness, with more than 30 percent of children with rare diseases dying before their fifth birthday. RAiN will help evaluate the quality of life and management of people living with rare diseases on the island of Ireland and internationally.
Commenting on the occasion of the launch, Taoiseach Leo Varadkar, TD said: “I am pleased to announce the launch of the All-Ireland Rare Diseases Interdisciplinary Research Network, which will strengthen cross border links between academic, clinical health, and social care researchers working to improve the lives of people affected by rare disorders. Through the RAiN network, researchers will work in partnership with patients and families to make real impacts in the day-to-day care, treatment and management for those living with conditions such as cystic fibrosis, PKU, chromosomal anomalies, and childhood cancers, and enhance cooperation in how we respond to these challenges on an all-island basis.”
Co-lead of RAiN for UCD, Associate Professor Suja Somanadhan said: “This all-Island interdisciplinary rare disease research network will serve as a hub to support collaboration and connection between members across the Island, which includes researchers, early career investigators, industrial partners and Public and Patient Involvement expert groups.”
Co-lead of RAiN for QUB, Professor Amy Jayne McKnight said: “I’m delighted that so many individuals in our local rare disease community have come together to establish this network and look forward to working in partnership with those working,
often on a shoestring budget, to improve the lives of people living with rare diseases.”
RAiN is funded by the Department of the Taoiseach from the Shared Island strand of Irish Research Council’s ‘New Foundations’ awards. The network builds on established north-south research partnerships between UCD and Queen’s*.
By fostering collaboration among researchers, practitioners, policymakers, patients and families working on rare diseases, RAiN will advance health service developments, leverage funding, and facilitate internationally excellent translational rare disease research.
Monthly seminars will discuss research that addresses the significant unmet health, social, psychological, and educational needs of children, young people affected by rare disease and their families. Nurtured research partnerships will inspire and empower early career researchers as emerging leaders for interdisciplinary rare disease research.
HOSPITAL SERVICES LIMITED (HSL) ANNOUNCES EXPANSION
Known for introducing innovative new health technologies to hospitals and healthcare facilities for the past 60 years across the island of Ireland, Hospital Services Limited (HSL) have expanded into

the UK with the launch of their new headquarters in the East Midlands, England, with the £1.7m investment aiming to grow the company’s footprint in the UK over the coming years.
A specialist distributor of medical and surgical equipment, consumable products, and healthcare IT solutions, HSL is one of the largest privately-owned distributors supplying the health sector in the UK and Ireland. In addition to supplying market leading technologies and solutions to its customers, HSL’s team provides on-going technical and clinical support to the end-user of our products.
HSL partners exclusively with many world-class manufacturers across several disciplines including, to name just a few, Richard Wolf and DTR Medical (general surgery), Hologic (mammography), Shimadzu (radiology), Fujifilm (endoscopy), and Haag-Streit and Ziemer (ophthalmology).
With financial backing from the Foresight Group, a leading independent infrastructure and private equity investment manager with over £6.5 billion of assets under management, HSL continues to grow its offering, both locally and across the UK, enabling its customers to focus on what is most important - the Patient.
Following continued growth and success in the UK where HSL
have established a reputation for supplying innovative, efficiencygrowing and high-quality radiology and healthtech, HSL have established a Britain-based team of 25 based across their new Draycott headquarters, an office in Bath, and positioned remotely across the regions of the UK including Wales.
The company also has ambitious plans to grow the team by at least 60% in the coming years through planned acquisitions and ongoing recruitment campaigns and has recently appointment Steve Leatherland as Regional Director of Operations in the UK. Commenting on his role in helping strategic growth for HSL Steve Leatherland said, “These are exciting times for HSL with a growing portfolio, an expanding team, and a working environment focused on creating a culture of customer centricity. With over 20 years’ experience in the healthcare service sector, I am looking forward to working with some of the best people and products in the marketplace.”
PHARMACYNEWSIRELAND.COM 80 Clinical Profiles
Graham Stewart, Commercial & Finance Director and Sam McMaster, Director of Telehealth photographed in HSL’s newly-opened Draycott headquarters
DUPIXENT® (DUPILUMAB) APPROVED BY EUROPEAN COMMISSION AS THE FIRST AND ONLY TARGETED MEDICINE INDICATED FOR EOSINOPHILIC ESOPHAGITIS
The European Commission (EC) has expanded the marketing authorization for Dupixent® (dupilumab) in the European Union (EU) to treat eosinophilic esophagitis (EoE) in adults and adolescents 12 years and older, weighing at least 40 kg, who are inadequately controlled by, are intolerant to, or who are not candidates for conventional medicinal therapy. EoE is a chronic, progressive inflammatory disease that damages the esophagus and prevents it from working properly. With this approval, Dupixent is the first and only targeted medicine specifically indicated to treat EoE in Europe and the U.S.
Naimish Patel, M.D. Head of Global Development, Immunology and Inflammation at Sanofi said, “The impact of EoE on a patient’s daily life cannot be overstated – the narrowing and scarring of the esophagus can make something as simple as eating a painful and distressing experience, and may lead to choking and food impaction. With this latest approval for Dupixent, adults and adolescents in the EU suffering from the chronic and often debilitating symptoms of EoE now have the first and only targeted treatment option clinically proven to reduce both esophageal inflammation and damage, as well as improve swallowing ability, pain and health-related quality of life.”
George D. Yancopoulos, M.D., Ph.D. President and Chief Scientific Officer at Regeneron added, “This latest approval establishes Dupixent as the only targeted medicine specifically indicated for eosinophilic esophagitis in the European Union. Dupixent is also the only biologic shown in pivotal trials to help patients achieve histological remission, reduce difficulty swallowing and improve healthrelated quality of life – all of which are crucial to reducing the burden of this debilitating disease. Since its first approval, Dupixent has redefined the treatment of certain chronic diseases with underlying type 2 inflammation and is now indicated for five conditions in the European Union. We remain committed to investigating Dupixent’s potential in additional diseases in which IL-4 and IL-13 may play a key role.”
The EC decision is supported by 52-week data from a Phase
3 trial consisting of three parts (Part A, B and C). Part A and Part B investigated Dupixent 300 mg weekly (Part A n=42; Part B n=80) compared to placebo (Part A n=39; Part B n=79) for 24 weeks. Part C (n=188) observed patients who had continued on or switched to Dupixent from Parts A and B for an additional 28 weeks.
Dupixent patients in Parts A and B, respectively, experienced:
• An approximately 10 times higher rate of histological disease remission (60% and 59%), a co-primary endpoint, compared to placebo (5% and 6%).
• A 69% and 64% reduction in disease symptoms compared to 32% and 41% with placebo. Disease symptoms were measured using the Dysphagia Symptom Questionnaire (DSQ), on which Dupixent patients experienced a 21.9- and 23.8-point clinically meaningful improvement compared to a 9.6- and 13.9-point improvement for placebo, a coprimary endpoint. Swallowing improvement was observed as early as four weeks.
• A greater than seven-fold reduction in abnormal endoscopic findings from baseline (-3.2 and -4.5 points) compared to placebo (-0.3 and -0.6 points).
• Nominally significant improvements in swallowingrelated pain and health-related quality of life, as well as less frequent non-swallowing symptoms.
Histological disease remission, swallowing improvement and reduction in abnormal endoscopic findings were consistent with the overall population in patients who were uncontrolled, or not responsive to or not eligible for swallowed topical corticosteroids. Longer term efficacy in Part C was similar to results observed in Parts A and B.
The safety results of the trial were generally consistent with the known safety profile of Dupixent in its approved indications. The most common side effects across indications include injection site reactions, conjunctivitis, conjunctivitis allergic, arthralgia, oral herpes and eosinophilia. Adverse events more commonly observed in EoE patients treated with Dupixent (n=122) compared to placebo (n=117) included infections (32% vs. 25%). An additional adverse reaction of injection site bruising was reported
in the EoE trial. The safety profile through 52 weeks was generally consistent with the safety profile observed at 24 weeks.
PORTIUNCULA UNIVERSITY HOSPITAL LAUNCHES ‘LITTLE JOURNEY’ APP FOR CHILDREN
Portiuncula University Hospital has launched the ‘Little Journey’ virtual reality app to help children between the ages of 3 and 12, to prepare for surgery and allay their anxiety in advance of their hospital stay.
The ‘Little Journey’ app provides 360 degree views of all the areas the children will visit at the hospital as well as useful information about anaesthesiology tailored to the age of the child.
Dr Vinod Sudhir, Consultant Anaesthesiologist at Portiuncula University Hospital said, “Preoperative anxiety in children and parents is a very real phenomenon before undergoing general anaesthesia. As healthcare professionals we recognise the increasing impact of anxiety and the physiological negative impact it can have on the child’s and parent’s ability to cope with events surrounding the experience of anaesthesiology and surgery.
“Children may have anxiety around the multidisciplinary environment of theatre, their expectation of events, meeting unfamiliar people and even fear of pain. Parents/ guardians can accompany their young children to theatre and be present with them during induction of anaesthesia. Some of the parent’s anxiety comes from their fear of the unknown and the steps surrounding their role with their child at the time their child undergoes anaesthesia. By providing information through the app, which uses child-friendly animation, we can begin to prepare parents/guardians and children for surgery and ease their distress.
“The ‘Little Journey’ app was developed to help change the way children experience hospitals by empowering them and giving them the information they need to reduce their anxiety in a fun, interactive format. The app helps children to familiarise themselves with the hospital and the handy checklists included will help families to prepare in advance of the hospital stay.
“Last year the demand for general anaesthetic increased in children due to the increase of paediatric day case surgery at the hospital. We want to help alleviate any distress due to anxiety whether the child is presenting for surgery or investigative procedures.”
The ‘Little Journey’ app is free to download from Google Play Store or App Store. It can be used on a smartphone in 2D or using a 3D virtual reality headset. The app gives children the chance to meet the animated healthcare characters who will explain what they do and what happens on the day of surgery, see some of the equipment which will be used to care for them, find out more about what to expect on the day of their procedure and includes a virtual tour of the children’s day ward, the theatre room and the recovery room at Portiuncula University Hospital.
Portiuncula University Hospital launches ‘Little Journey’ virtual reality app to help children between the ages of 3 and 12, to prepare for surgery and allay their anxiety in advance of their hospital stay. From left, Elizabeth Fitzgerald, Theatre Staff Nurse; Breda Brady, Clinical Skills Facilitator, Paediatric Unit; 6 year old Diarmuid Fallon from Oran, County Roscommon and Dr Vinod Sudhir, Consultant Anaesthesiologist

PHARMACYNEWSIRELAND.COM 81
JANSSEN PRESENTS UPDATED DATA DEMONSTRATING IMPROVED OUTCOMES FROM THE USE OF NIRAPARIB IN COMBINATION WITH ABIRATERONE ACETATE PLUS PREDNISONE AS A FIRST-LINE THERAPY IN PATIENTS WITH BRCA-POSITIVE METASTATIC CASTRATION-RESISTANT PROSTATE CANCER
The Janssen Pharmaceutical Companies of Johnson & Johnson has announced updated results from the Phase 3 MAGNITUDE study evaluating the investigational use of niraparib, a highly selective poly (ADP-ribose) polymerase (PARP) inhibitor, in combination with abiraterone acetate plus prednisone (AAP) in patients with metastatic castration-resistant prostate cancer (mCRPC) with or without specific homologous recombination repair (HRR) gene alterations, including BRCA mutations.1 Results will be featured in a Rapid Abstract Session (Abstract #170) at the American Society of Clinical Oncology’s Genitourinary (ASCO GU) Cancers Symposium 2023, taking place February 16-18.1
In the second interim analysis (IA2) of the MAGNITUDE study (NCT03748641), the treatment combination of niraparib and AAP, in comparison to placebo and AAP at 26.8 months of median followup, demonstrated a statistically significant prolongation in time to symptomatic progression (TSP) and continued consistent improvement of time-to-initiation of cytotoxic chemotherapy (TCC) in the HRR-positive population and a strong improvement in TSP for the BRCA subgroup of the HRR-positive population.1,2 Updated radiographic progression free survival (rPFS) results were consistent with the primary analysis which showed statistically significant benefit in both the HRRpositive population and BRCA subgroup.1,2,3 Additionally, a trend toward improvement in overall survival (OS) was observed in the BRCA subgroup.1,2 No new safety signals were identified.1,2 The most common adverse events for niraparib and AAP versus placebo and AAP, regardless of causality, were anemia (50.0 percent vs 22.7 percent, respectively), hypertension (33.0 percent vs 22.3 percent) and constipation (33.0 percent vs 15.6 percent).1,2 Patients without HRR gene alterations had no improvement in outcomes from the use of niraparib in combination with AAP.1,2
Notably, in the BRCA subgroup (8.1 months additional follow-up at IA2), rPFS by central review
demonstrated a consistent and clinically meaningful treatment effect favoring niraparib and AAP, with a median rPFS of 19.5 months at IA2 compared with 10.9 months for placebo and AAP (hazard ratio [HR], 0.55 (95 percent confidence interval [CI], 0.39-0.78).1,2 For patients with BRCA-positive mCRPC, preplanned sensitivity analysis evaluating rPFS by investigator review also showed benefit for niraparib and AAP (HR, 0.46 [95 percent CI, 0.32-0.67]).1,2 Further, results of the IA2 indicate that patients with BRCA mutations treated with niraparib and AAP experienced a trend towards delayed time to worst pain intensity (HR, 0.70 [95 percent CI, 0.44-1.12]) and pain interference (HR, 0.67 [95 percent CI, 0.40-1.12]) compared with placebo and AAP.1,2
“At Janssen, our goal is to provide treatment options that delay progression, prolong life, and support a better quality of life for those diagnosed with prostate cancer,” said Martin Vogel, EMEA Therapeutic Area Lead for Oncology, JanssenCilag GmbH. “The MAGNITUDE study highlights the importance of biomarker testing to identify those who will optimally benefit from the combination of niraparib and AAP. This is a crucial step in ensuring we can bring the right treatment to the right patients, based on their unique characteristics, and speaks to our wider commitment to exploring precision medicine to treat, intercept and prevent, and potentially one day cure, diseases like mCRPC.”
Prostate cancer is the most common cancer in men across Europe.4 In 2020, more than 473,000 patients were diagnosed in Europe and over 100,000 deaths were attributed to this challenging disease.5 Patients with mCRPC and HRR gene alterations, of which BRCA mutations are the most common, are more likely to have aggressive disease, poor outcomes and a shorter survival time.6,7,8,9 Up to 30% percent of mCRPC cancer cases have alterations in genes associated with HRR.3,10 Approximately 10 to 15 percent of patients with mCRPC have BRCA gene alterations.11,12
In April 2022, Janssen submitted a marketing authorisation application to the European Medicines Agency seeking approval for niraparib in combination with abiraterone acetate in the form of a dual action tablet (DAT), plus prednisone or prednisolone, based on data from the MAGNITUDE study.13 Marketing authorisation applications are under review across a number of countries globally.
EXAMINING RISE IN HEALTHRELATED CLAIMS
Minister for Health Stephen Donnelly has received government approval to establish an Interdepartmental Working Group to examine the rising cost of health-related claims and consider mechanisms to reduce costs. The Group will examine the rising cost of clinical negligence claims in the health system, with a particular focus on high value claims, and identify measures that could be put in place to reduce future costs.
The Group’s considerations will include developing a plan to implement risk management and other initiatives to reduce the occurrence of adverse incidents and to recommend measures to address patient concerns following the occurrence of adverse incidents, taking into account measures suggested by Dr Scally in his final implementation review report.
The Group will be chaired independently by an expert healthcare professional, Dr Rhona Mahony and will be comprised of membership from across key government departments and agencies.
Minister Donnelly stated:
“The most effective way to manage the cost of claims against the HSE is to minimise incidents of avoidable harm. While the department and the HSE work continuously to monitor and improve patient safety, reduce incidents of harm and to minimise risk, I am keen to take further action on this.
“The establishment of this Group, chaired by, Dr. Rhona Mahony and comprising membership from across key government departments and agencies, will be essential in identifying measures that could be put in place to improve outcomes for patients and reduce future costs. This is an important piece of work for patients and for the whole health service and I look forward to receiving the group’s findings and recommendations in due course.”
NEW PATIENT ADVICE AND LIAISON SERVICE COORDINATOR FOR LETTERKENNY UNIVERSITY HOSPITAL

Letterkenny University Hospital is delighted to announce the appointment of Angela Mc Closkey to the role of Patient Advice and Liaison Service (PALS) Coordinator. Angela is from Letterkenny and spent 19 years working as a Radiographer in Letterkenny
University Hospital prior to her appointment as PALS Coordinator.
The Patient Advice and Liaison Service Coordinator acts as a visible focal point for patients, families and carers and is often the main contact within the hospital. They help to resolve issues for patients and their families and work towards improving the patient experience at any available opportunity.
Speaking about her appointment Angela said; “Within the hospital every contact we have with a patient can have a lasting impact and I try and make that contact as positive as possible. My role involves ensuring that the patient voice is heard either through the patient directly or through a nominated representative.
“If a patient wants to provide feedback or make a comment about the hospital and the care they received, I can assist them in doing so, or refer them to the appropriate person who will be able to assist them further.”
Sean Murphy, General Manager at Letterkenny University Hospital added; “This is the first appointment of a PALS Coordinator to Letterkenny University Hospital and I am delighted to welcome Angela to the role. PALS Coordinators have a very important function as they help to embed the voice of the patient in the workings of the hospital. Patients are at the centre of everything we do and through the PALS service we can learn more about the patient experience and put plans in place to make necessary improvements.”
ALLCARE PHARMACY ANNOUNCE NEW SPONSORSHIP
RTÉ Media Sales has announced Allcare Pharmacy as the new sponsor of Today with Claire
PHARMACYNEWSIRELAND.COM 82
Clinical Profiles
Angela Mc Closkey (PALS)
Byrne, RTÉ Radio 1, Monday –Friday, 10am-12pm.
Brokered by Javelin, the 11-month RTÉ Radio 1 sponsorship includes 6 x 10-second sponsor-credited stings per show, sponsorcredited promos in Rising Time, Liveline, Drivetime, Saturday with Colm O’Mongain and Brendan O’Connor as well as podcast and homepage sponsorship.
Today with Claire Byrne is currently joint seventh most listened-to radio programme in the country, with a daily audience of 344,000.
Caroline Burton, Head of Retail Marketing at Uniphar Group said “Allcare Pharmacy is delighted to partner with Claire Byrne and RTE Radio 1 in 2023. As Ireland’s largest community pharmacy network, it was important for us to find a partner which reflects the informative, entertaining and important topics of the day that matter to our customers. Today with Claire Byrne is a perfect fit for a trusted community pharmacy brand like Allcare Pharmacy.”

SAXENDA® (LIRAGLUTIDE 3MG) INJECTION APPROVED FOR REIMBURSEMENT IN IRELAND FOR ADULTS LIVING WITH OBESITY
Novo Nordisk have announced that Saxenda® (liraglutide 3mg) has been granted reimbursement in Ireland for the treatment of adults living with obesity.1 Liraglutide 3mg is the only obesity medicine reimbursed for people with an initial Body Mass Index (BMI) of ≥35kg/m2, pre-diabetes and at least one cardiovascular risk factor, in combination with a reduced calorie diet and increased physical activity.1,2
While people living with obesity may have been advised to ‘eat less
and move more’, clinical guidelines recommend moving beyond this simplistic approach to address the root drivers of obesity.6 Instead, people living with obesity should have access to evidence-informed interventions, including medical nutrition therapy, physical activity, psychological interventions, pharmacotherapy and surgery.6
Professor Donal O’Shea, HSE Clinical Lead for Obesity said: “Today’s announcement of liraglutide 3mg reimbursement for obesity, represents a landmark moment in Ireland’s changing response to how obesity is managed following the introduction of a new HSE Model of Care for the Management of Overweight and Obesity last year. Liraglutide 3mg has demonstrated, both in clinical studies and real-world use, clinically meaningful weight loss when combined with diet and exercise.”7-12
Liraglutide 3mg, a human glucagon-like peptide-1 (GLP1) analogue, comes in pre-filled pens as a once daily injection. Reimbursement is through a managed access protocol, run by the HSE’s Medicines Management Programme, and those qualifying for reimbursement will need to satisfy the following eligibility criteria: Body Mass Index (BMI) of ≥35kg/m2, pre-diabetes and at least one cardiovascular risk factor. For full details on reimbursement criteria, please see: https://www. hse.ie/eng/about/who/cspd/ncps/ medicines-management/managedaccess-protocols/liraglutidesaxenda-/. For people living with obesity who do not meet these criteria, the medicine can still be prescribed and purchased at the individual’s expense.
Treatment with Liraglutide 3mg should be discontinued after 12 weeks on the 3mg/day dose if people have not lost at least 5% of their initial body weight.2 Further prescribing information can be found at: https://www.medicines. ie/medicines/saxenda-6-mg-mlsolution-for-injection-in-pre-filledpen-34785/spc
UCD RUGBY CLUB TO RAISE FUNDS FOR IRISH CANCER SOCIETY DAFFODIL DAY

UCD Rugby Club, sponsored by EY Ireland, has announced details of their fundraising drive to raise vital funds for the Irish Cancer Society’s annual Daffodil Day.
UCD Rugby Club made the announcement at the UCD Bowl.
Averil Power, CEO Of the Irish Cancer Society, said, “We are grateful to UCD Rugby Club for the incredible effort that they’ve put in
every year to run Daffodil Day on the UCD campus. We are also so grateful to our wonderful partners in EY for their support. The Irish Cancer Society typically gets three percent of our funding from the State. Therefore, we have to raise over twenty-five million euro every year to fund all of our free nursing, counselling and transport to cancer treatment, as well as our life-saving and life-changing cancer research and trials. We genuinely couldn’t provide all of the vital services that we do without the support of UCD Rugby Club and EY.”
Graham Reid, EY Ireland Partner and Head of Markets, added, “EY are very proud to support UCD RFC’s fundraising drive for The Irish Cancer Society, which is also EY Ireland’s Charity Partner this year. The Irish Cancer Society is an incredible community of patients, survivors, volunteers, supporters, health, social care professionals and researchers offering free care, advice and support for cancer patients and their loved ones. Their vision is that, by 2025, three out of every four cancer patients in Ireland will survive their diagnosis and, in future, no one in Ireland will die from the disease. We in EY want to play our part in helping them achieve that vision through fundraising and raising awareness of the signs, symptoms, and importance of early detection with all our people.”
Strength in numbers – Players and representatives from UCD Rugby Football Club are joined by representatives from The Irish Cancer Society and EY for the launch of their annual daffodil day fundraising drive in aid of The Irish Cancer Society
PHARMACYNEWSIRELAND.COM 83
Pictured L-R are Caroline Burton, Head of Retail Marketing at Uniphar Group, Geraldine O’Leary, Commercial Director, RTÉ, and Aoife Hofler, Director, Javelin
www.smahcp.ie/infant-health
IMPORTANT NOTICE: Breastfeeding is best. SMA® Xpert ProCol is not a substitute for breast milk and does not replace o balanced diet. Before using any dietary supplement, please discuss with your healthcare professional. Food supplements should not be used as a substitute for a balanced and varied diet or healthy lifestyle. Do not exceed the recommended doily dose. Keep out of reach of children. SMA® Xpert ProHydrate must be used under medical supervision. SMA® Xpert ProHydrate is intended for the dietary management of gastroenteritis. It is suitable for infants (0-12 months) and children (1-3 years). If the condition does not improve within 24-48 hours of starting SMA® Xpert ProHydrate, the family doctor should be consulted. SMA® Xpert ProHydrate is not suitable for use as the sole source of nourishment. For Enteral Use Only. Always follow medica l advice. For babies, always hold them while feeding and do not leave them unattended as they might choke.

ZTC5873a/07/22 | JU001, ITNUB019, ITNU004
SMA® Nutrition Ireland. ®Reg. Trademark of Société des Produits Nestle S.A.






