
This briefing examines health outcomes for migrants (defined as people who were born abroad) as well as the extent to which health problems impact their day-to-day activities or their jobs. It also looks at the health-related factors that increase the risks of some migrant communities of becoming seriously ill from COVID-19.
This briefing will be updated when the Census 2021 data are released
-
Key Points
- Migrants are healthier, on average, than the UK born. In 2019, 27% of the foreign-born population said that they had a long-lasting health problem; this is 15 percentage points lower than the UK born (42%).
More… - Migrant workers in low-skilled jobs were more likely to say that they had a long-term limiting health problem than those in high-skilled occupations.
More… - Migrants who have lived in the UK for longer are more likely to have health problems than those who arrived recently, even when comparing people in the same age groups.
More… - The share of residents reporting a long-lasting mental health problem is 5% for the foreign born and 10% for the UK born.
More… - Foreign-born men are more likely to smoke than UK-born men, while the opposite is true among women.
More… - The prevalence of underlying health conditions that increase the risk of becoming very ill from COVID-10 varies across migrant communities.
More…
- Migrants are healthier, on average, than the UK born. In 2019, 27% of the foreign-born population said that they had a long-lasting health problem; this is 15 percentage points lower than the UK born (42%).
-
Understanding the Evidence
This briefing examines the outcomes of people who were born abroad and have migrated to the UK. The word ‘migrant’ is used differently in different contexts. In this briefing, we use the term ‘migrant’ to refer to the foreign born, regardless of whether they have become UK citizens. ... Click to read more.For a discussion of this terminology, see the Migration Observatory briefing Who Counts as a Migrant: Definitions and their Consequences.
This briefing relies on the Labour Force Survey (LFS) quarterly data from 2019, the Annual Population Survey (APS) from 2019, and Understanding Society: COVID-19 Study, 2020 (First wave, April 2020). The LFS and APS collect data on respondents’ self-reported health as well as on relevant sociodemographic characteristics and labour market situation. The Understanding Society COVID-19 Study includes all members of the main Understanding Society survey and covers the changing health, economic and social impacts of the COVID-19 pandemic on respondents. In all three surveys, only respondents’ who are aged 16 or older are asked the questions included in the health modules. Because health data are self-reported, it is possible that certain health conditions are misreported.
The LFS is the largest household study in the UK (39,000 households) and provides the official measures of employment and unemployment. It collects information about a wide range of topics on individuals above age 15 every quarter. The APS includes most of the same individuals as the LFS but also includes and additional boost to the sample. Some variables are not available in the APS, however, and in those cases this briefing uses the LFS instead. The LFS/APS have some important limitations. Some people are excluded, such as residents of communal establishments like hostels, and other groups may be undercounted due to survey non-response. Its response rate has declined over time, and is now below 50% (ONS, 2016); this means that people who are more likely not to respond to the survey may be undercounted. ONS analysis based on the Census suggests that non-response is a greater problem among people born outside of the UK (Weeks et al, n.d.). The fieldwork of the first wave of the Understanding Society COVID-19 study took place in April 2020 and the response rate was 38.7%. Weights are provided to adjust for unequal selection probabilities and non-response.
Health variables used in this briefing
The health data presented in this briefing is self-reported and refers to long-lasting health problems; that is, physical or mental health conditions or illnesses that are lasting or are expected to last at least 12 months. Under the Equality Act 2010, health conditions may be considered a disability if they have a substantial adverse effect on the person’s ability to carry out normal day-to-day activities for at least 12 months (Equality Act 2010: Chapter 1 Section 6).
In the LFS, respondents reporting a long-lasting health problem give information about the extent to which their health problem affects their ability to carry out day-to-day activities (not at all, a little, or a lot). This briefing uses the term limiting health problem when the respondent has said that the health problem limits their daily activities either a little or a lot. It uses the term non-limiting health problem when they have said that they have a long-lasting health condition that does not limit their daily activities.
The Understanding Society COVID-19 study includes a module where respondents report whether they have at least one underlying health condition that increases their risk of becoming very ill with COVID-19. The list of conditions included in this survey module is very comprehensive and reflects the NHS guidelines on people at higher risk from coronavirus (NHS, 2020).
Data breakdowns
In addition to country of birth, most data breakdowns include individuals’ age, which is a key determinant of their health. Both biological and social determinants have to be acknowledged in any analysis comparing the health of the foreign and the UK born, as these factors will differ across the two groups.
The briefing presents data for the UK-born and foreign-born populations either as a whole or for different country of birth groupings. About 40% of migrants in the UK were born in the EU and around a quarter were born South, East or Southeast Asian countries. See the the Migration Observatory briefing Migrants in the UK: an overview for more information about the geographic origins of the foreign born population.
When considering the skill level associated with a person’s job, this briefing uses a four-part classification based on the amount of training required, developed by the Office of National Statistics (ONS, 2010). This classification distinguishes between low-skilled, medium-low skilled, medium-high skilled and high-skilled occupations.
Margins of error in the estimates
Because the LFS, APS and Understanding Society are sample surveys, the estimates come with margins of error. This means that small differences between numbers or percentages may not be statistically significant. However, all the differences between groups that are described in the text of the briefing are all statistically significant. A difference between two groups is considered statistically significant when the probability that this difference is caused by chance is very small. In that case, we assume that the differences we observe in the data are likely to exist in the population. Note that small differences between estimates for different groups may not be statistically significant, if they are not described in the narrative of the briefing.
Migrants in the UK were less likely to have health problems than the UK born, according to survey data from 2019
Migrants’ health is shaped by a wide range of factors, ranging from their pre-migration experiences; their experiences during and after migration to the UK; their work, education and socio-economic status; and their ethnicity, which affects the prevalence of certain health conditions.
Studies on the health of the migrant and non-migrant populations have typically shown that the foreign born are, on average, healthier than non-migrants (e.g. Jasso et al., 2004; Antecol and Bedard, 2006). Those who decide to migrate tend to be younger and healthier than those who stay behind and, at the same time, the heathiest migrants are more likely to stay in their new destination rather than returning to their origin countries. This produces a ‘migrant health advantage’, a phenomenon that researchers have referred to as the Healthy Immigrant Effect.
Despite this general trend, the migrant population is made up of many different groups with different characteristics, and some groups might have worse health outcomes than the average. For example, people who migrated for employment, family and study reasons have better health than the UK born, while those who migrated to seek asylum have worse health outcomes (Giuntella et al., 2018). In addition to refugees and asylum seekers, there might be other vulnerable groups with special health needs within the migrant population, whose outcomes will not be clearly visible when looking at averages in the data.
Overall, migrants in the UK are healthier than the UK born population. In 2019, 27% (2,297,000) of the foreign-born population in the UK said that they had a long-lasting health problem (including both limiting and non-limiting conditions – see understanding the evidence), which was 15 percentage points lower than the UK born (42%). The migrant health advantage over the UK born is largest with regard to limiting health problems – that is, health problems that limit respondents’ day-to-day activities (Figure 1).
This difference is in part explained by the fact that the foreign born are on average younger, e.g. 88% of those born abroad were below age 65, compared to 76% of the UK born. But even within the same age groups, the foreign born are healthier than the UK born, at least among the population below age 50 (Figure 1). For example, the share of those aged 16 to 34 reporting a long-lasting health problem, including both limiting and non-limiting health conditions, was 12 percentage points lower for the foreign born than for the UK born.
Figure 1
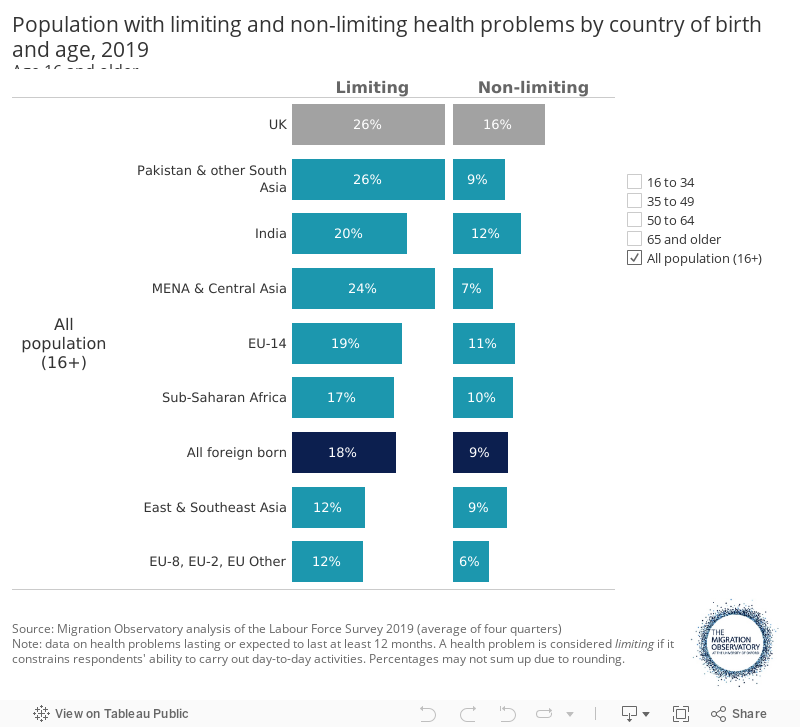
Health varies widely by country of origin. For example, migrants from the new EU accession countries and East and Southeast Asia have the lowest shares with health problems that limit daily activity. (Figure 1). People born in Pakistan and other South Asian countries (excluding India) below age 35 report fewer limiting health problems than the UK born (8% vs 16%), though their health is worse than the latter among the older age groups. For example, the share of Pakistanis and other South Asians with limiting health problems is around 17 percentage points higher than for the UK born among the population aged 50 to 64. Among this age group, people born in Pakistan and other South Asian countries (excluding India) were more likely to report diabetes as their main health condition (16% of those with a long-lasting health problem) compared to the UK born (3% of those with a long-lasting health problem). The high prevalence of type 2 diabetes among South Asians has been attributed to both biological and contextual factors (Gujral et al., 2013).
The migrant health advantage over the UK born is larger among workers with limiting health conditions in low-skilled occupations
It is widely recognised that people with higher incomes or other measures of socio-economic status have better health outcomes (Elo, 2009). The reasons for this are complex and not just explained by a single factor. Some low-skilled jobs increase the risk of experiencing health problems (Pampel et al., 2010) because they are physically intensive and have poor working conditions (e.g. cleaning, construction), or because low incomes mean that they are less able to purchase goods and services to improve their health (Benzeval et al, 2014). In addition, people that are unable to move out of low-skilled and low-paid jobs are more likely to experience chronic stress due to their socioeconomic situation (Layte & Whelan, 2014), which ultimately affects their overall health. Causation may also run the other way: poor health may affect economic outcomes if it limits people’s ability to work.
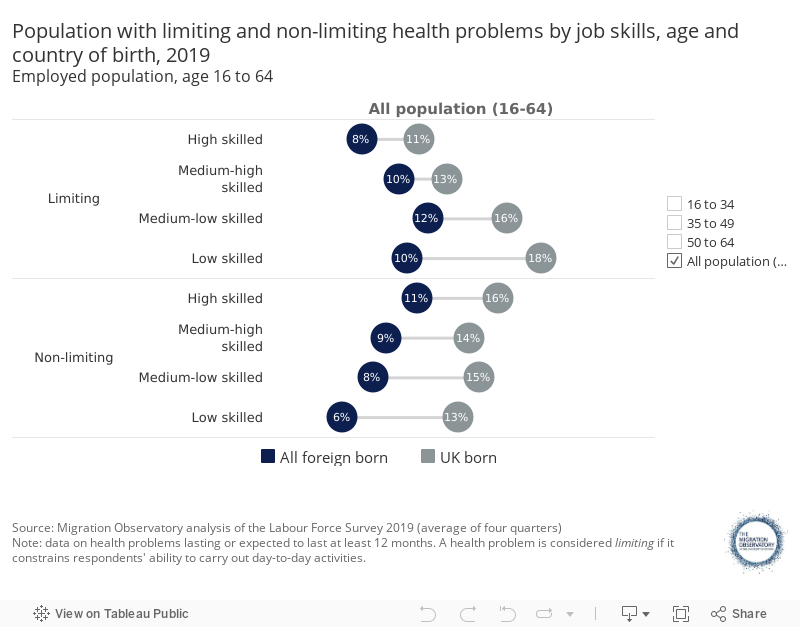
Both migrants and the UK born in high-skilled jobs are less likely to say they have a limiting health problem than those in low-skilled jobs; the difference in limiting health problems between workers in low- and high-skilled jobs is, however, more pronounced among UK-born workers (Figure 2). There is no clear relationship between the skill categorisation of the job and health for non-limiting health problems.
Although the health advantage of the foreign born over the UK born is apparent for both limiting and non-limiting health conditions, this advantage is larger among workers with limiting health conditions in low-skilled occupations. For example, among workers in low-skilled jobs aged 35 to 49, 20% of the UK born report a limiting health condition, while this share is 11% among migrants – a gap of 9 percentage points; however, among people in high-skilled jobs, the gap between migrant and UK-born workers is of 3 percentage points (Figure 2).
Figure 2
Note that these figures only include people who are working, either as employees or self-employed, and thus excludes people who cannot work. There is evidence, for example, that poor health outcomes among asylum seekers may reduce their labour market participation (Kone et al, 2019).
Migrants’ health advantage over the UK born is larger for those who recently moved to the UK
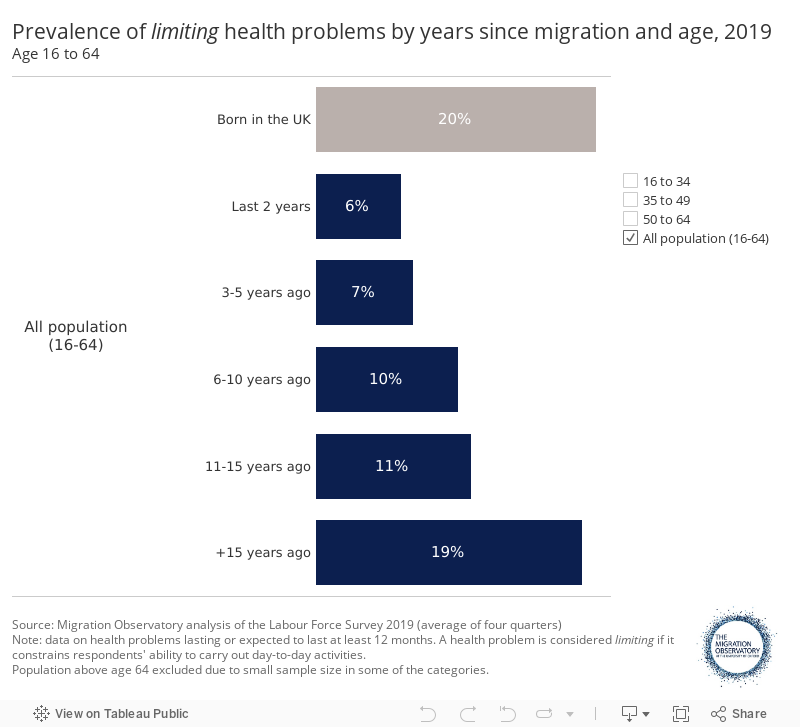
Despite the initial health advantage of the migrant population, their health tends to converge to that of the UK born as their time spent in the UK increases (Figure 3). Note, however, that Labour Force Survey data does not follow the same individuals over time; it is thus possible that the health advantage of recently-arrived migrants results from other factors such as return migration of those with worse health outcomes or changes in the profile of people who migrate to the UK at different points in time.
Only 6% of people who migrated to the UK in the last 2 years say they have a limiting health problem, but this rises to 11% for those that moved between 11 and 15 years ago (Figure 3). The share for the foreign born that moved more than 15 years ago, at 19%, is similar to that of the UK born (20%). The convergence towards the UK born as the years of residence in the UK increase is not as stark for all age groups. Among 16 to 34 year olds, in particular, migrants still have a notable health advantage after 15 years.
Figure 3
The share of the population reporting a long-lasting mental health problem is 10% among the UK born and 5% among the foreign born
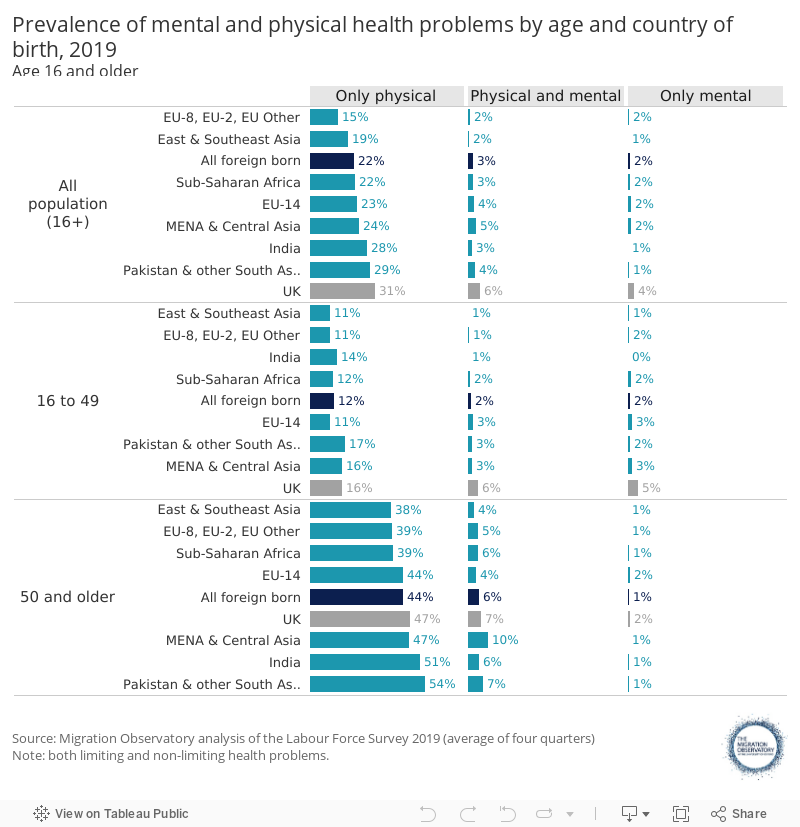
In general, it is more common to have both a mental and a physical health condition at the same time than a mental health condition alone (Figure 4), which suggests that there could be a relationship between both, e.g. certain illnesses might affect people’s quality of life, hence impacting their psychological wellbeing.
Overall, the share of population saying they have a long-lasting psychological condition (depression or other type of mental illness) is 10% for the UK born and 5% for migrants (425,000) (Figure 4). The prevalence of mental health problems is the highest among people older than age 50. Among this age group, the highest prevalence is found among the population born in Middle East, Central Asia and North African countries (11%), the UK born (9%) and among the population born in Pakistan and other South Asian countries (8%).
Figure 4
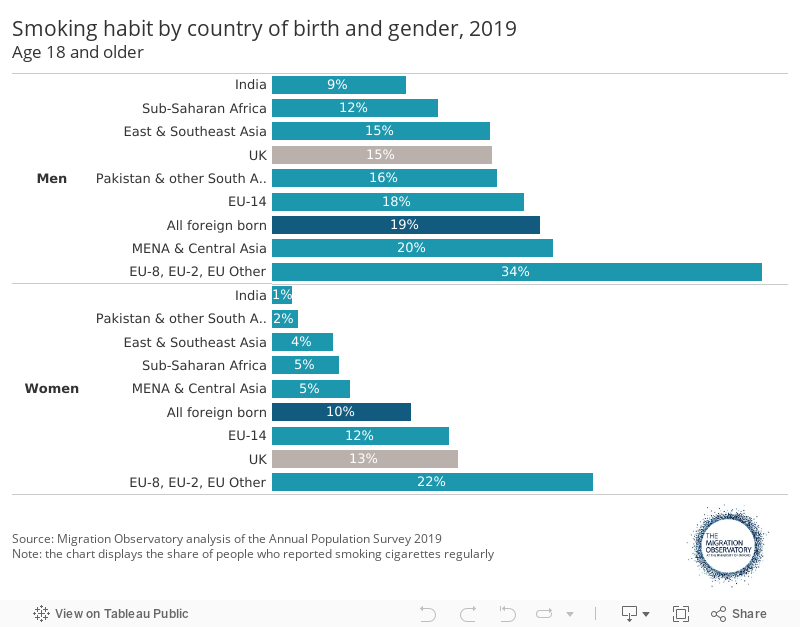
Foreign-born men are more likely to smoke than UK-born men, but the opposite is true among women
Smoking is a major risk factor for health. Overall, women are less likely to smoke than men and this is true of both migrants and the UK born (Figure 5). However, migrant women are less likely to smoke than UK-born women (10% vs. 13%). The opposite is true when comparing foreign-born men with the UK born (19% vs. 15%). Residents born in new EU accession countries have the highest share of smokers while those born in India have the lowest (Figure 5).
Figure 5
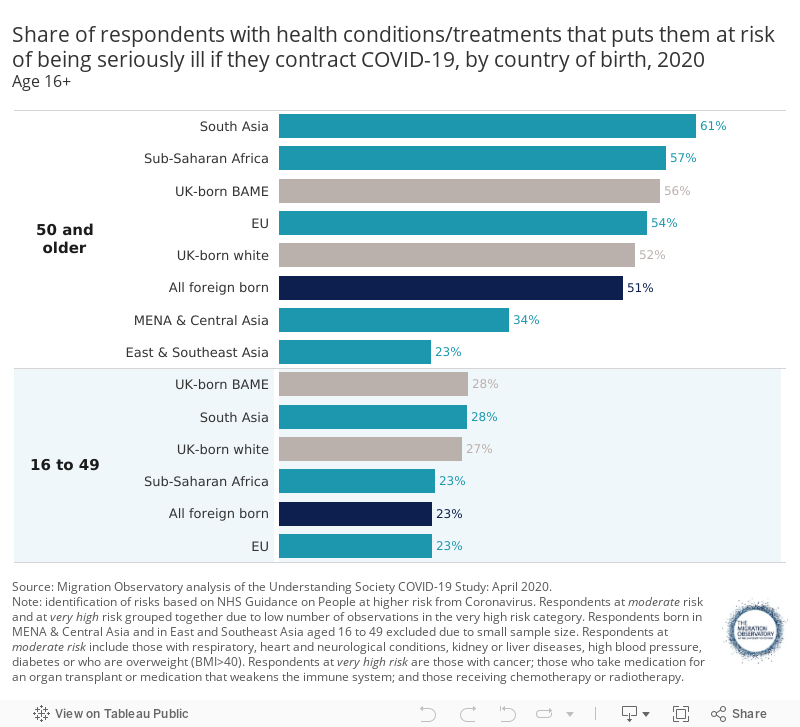
Among the population aged over 50, those born in East and Southeast Asia are less likely than UK-born whites to report health conditions that increase the risk of becoming very ill with COVID-19 (23% vs 52%)
As shown earlier, migrants are on average younger and report fewer long-term health conditions than the UK-born population of the same age group. As the worst impacts of COVID-19 have been concentrated at older ages (Beam Dowd et al., 2020), the UK’s migrant population has a demographic advantage in its age structure.
There is evidence that COVID-19 has had a disproportionate impact on black, Asian and minority ethnicity (BAME) communities, who have a higher mortality rate than the white British population once relevant social and demographic factors have been accounted for (Pan et al., 2020; Platt and Warwick, 2020). The foreign-born are a significant component of the UK’s non-white population – the Annual Population Survey 2019 showed that 50% of the BAME population in the UK were born abroad. Although differences across ethnic groups in mortality rates are partially related to both demographic and socio-economic characteristics, certain underlying health conditions that increase the severity of COVID-19 are more prevalent among older members of the Bangladeshi, Pakistani and black Caribbean communities than among the White-British population (Platt and Warwick, 2020).
Based on the NHS guidelines about people at higher risk from coronavirus (NHS, 2020), we can identify the migrant communities who are at very high risk or at moderate risk of becoming seriously ill with the disease due to their underlying health conditions (Figure 6). People at very high risk are mainly those undergoing cancer treatments or other medications that weaken the immune system; people at moderate risk are those reporting at least one of the following health conditions: respiratory, heart and neurological conditions, kidney or liver diseases, high blood pressure, diabetes or a BMI higher than 40. Figure 6 groups together these two risk groups due to low number of foreign-born respondents at very high risk.
Among the UK-born white population aged over 50, 52% of people are considered to be at risk. Among the population born in South Asia in the same age group, the share of those at risk rises to 61%, although the difference with respect to UK-born whites is not statistically significant. The South Asian disadvantage is, to a great extent, related to the high prevalence of type 2 diabetes among this group (Gujral et al., 2013). Other migrant communities aged over 50, however, are less likely than the UK-born white population to be at risk; for example, the share is 23% for over-50s born in East and Southeast Asian countries (Figure 6).
Figure 6
Evidence gaps and limitations
A drawback of survey health data is that they usually rely on self-reported measures instead of on objective indicators. Some other surveys, such as the UKHLS, have collected data on the bio-medical profile (e.g. blood pressure, weight, height, body fat, lung function, etc) of respondents sampled in the first wave of the survey. Unfortunately, this information has not yet been collected for the immigrant boost sample, as they were not part of the initial sample when the survey was launched. Collecting this type of health information for a large sample of the population is very expensive, as only qualified nurses can do it.
This briefing does not differentiate the foreign born population by reason of migration. Recent research has, however, shown that those who migrated for employment, family and study reasons have better health outcomes than the UK born, but this is the opposite for those who migrated to seek asylum (Giuntella et al., 2018).
There is limited quantitative information on how migrants engage with health services – for example, by registering with a GP or taking up preventative health services such as immunisation. The data in this briefing also does not tell us how migration affects expenditure on health care in the NHS. Given that migrants are on average younger and healthier than the UK born, they are expected to be less likely to use the NHS and thus account for less health expenditure per person than the UK born (Oxford Economics, 2018: 24). However, the costs of healthcare will depend not just on average health outcomes but also the specific conditions people have and any additional costs associated with treating them (e.g. due to language barriers, population churn and use of primary care services).
Acknowledgements
Thanks to Alita Nandi, Carlos Vargas-Silva, Jill Rutter and CJ McKinney for comments on an earlier draft of this briefing.
This briefing is part of the Migration Observatory’s Integration Initiative, which is funded by the Paul Hamlyn Foundation (PHF). The Paul Hamlyn Foundation is an independent funder working to help people overcome disadvantage and lack of opportunity, so that they can realise their potential and enjoy fulfilling and creative lives. This briefing was also made possible by the University of Oxford Social Science Division’s Economic, Social, Cultural and Environmental Impacts of Covid-19 – Urgent Response Fund.
References
- Antecol, H., & Bedard, K. (2006). Unhealthy assimilation: why do immigrants converge to American health status levels?. Demography, 43(2), 337-360. Available online
- Beam Dowd J., Andriano L, Brazel DM, Rotondi V, Block P, Ding X, Liu Y, Mills MC. (2020). Demographic science aids in understanding the spread and fatality rates of COVID-19. Proceedings of the National Academy of Sciences. 117(18): 9696-8. Available online
- Benzeval, M and Bond, L and Campbell, M and Egan, M and Lorenc, T and Petticrew, M and Popham, F (2014) How does money influence health? Joseph Rowntree Foundation. Available online
- Blanchflower, D., Costa, R., & Machin, S. (2017). The return of falling real wages. CEP Real Wages Updates, 6.
- Elo, I. T. (2009). Social class differentials in health and mortality: Patterns and explanations in comparative perspective. Annual Review of Sociology, 35, 553-572. Available online
- Equality Act 2010, c. 15 Available at: http://www.legislation.gov.uk/ukpga/2010/15/pdfs/ukpga_20100015_en.pdf
- Giuntella, O., Kone, Z. L., Ruiz, I., & Vargas-Silva, C. (2018). Reason for immigration and immigrants’ health. Public health, 158, 102-109. Available online
- Gujral, U. P., Pradeepa, R., Weber, M. B., Narayan, K. V., & Mohan, V. (2013). Type 2 diabetes in South Asians: similarities and differences with white Caucasian and other populations. Annals of the New York Academy of Sciences, 1281(1), 51-63. Available online
- Jasso, G., Massey, D. S., Rosenzweig, M.R. & Smith, J.P. (2004). Immigrant health: selectivity and acculturation (No. 04/23). IFS Working Papers, Institute for Fiscal Studies (IFS). Available online
- Kone, Z., Ruiz, I. & Vargas-Silva, C. (2019). Refugees and the UK Labour Market. COMPAS Working Paper. Available online
- Layte, R., Whelan, C. t. (2014) Who Feels Inferior? A Test of the Status Anxiety Hypothesis of Social Inequalities in Health, European Sociological Review, 30(4), 525–535, https://doi.org/10.1093/esr/jcu057
- Luthra, R., Nandi, A., & Benzeval, M. (2018). Unravelling the ‘immigrant health paradox’: ethnic maintenance, discrimination, and health behaviours of the foreign born and their children in England. Journal of Ethnic and Migration Studies, 1-22. Available online
- NHS (2020). Who’s at higher risk from coronavirus. Available online
- ONS (2010). Standard Occupational Classification 2010: Volume 1 Structure and descriptions of unit groups. Available online
- Oxford Economics (2019). The fiscal impact of immigration on the UK. A report for the Migration Advisory Committee. June 2018. Available online
- Palloni, A., & Arias, E. (2004). Paradox lost: explaining the Hispanic adult mortality advantage. Demography, 41(3), 385-415. Available online
- Pampel, F. C., Krueger, P. M., & Denney, J. T. (2010). Socioeconomic disparities in health behaviors. Annual review of sociology, 36, 349-370. Available online
- Pan, D., Sze, S., Minhas, J.S., Bangash, M.N., Pareek, N., Divall, P., Williams, C.M., Oggioni, M.R., Squire, I.B., Nellums, L.B. and Hanif, W. (2020). The impact of ethnicity on clinical outcomes in COVID-19: A systematic review. EClinicalMedicine, The Lancet, vol.23, 100404. Available online
- Platt, L., & Warwick, R. (2020). Are some ethnic groups more vulnerable to COVID-19 than others. Institute for Fiscal Studies, Nuffield Foundation. Available online
- University of Essex, Institute for Social and Economic Research. (2020). Understanding Society: COVID-19 Study, 2020. (April 2020) 2nd Edition. UK Data Service. SN: 8644, 10.5255/UKDA‐SN‐8644‐2. Available online
- Week, A., Fallows, A., Broad, P., Merad, S., & Ashworth, K. Non-response Weights for the UK Labour Force Survey? Results from the Census Non-response Link Study. Survey Methodology and Statistical Computing, Office for National Statistics. Available online