
Tolerability of Oral Supplementation with Microencapsulated Ferric Saccharate Compared to Ferrous Sulphate in Healthy Premenopausal Woman: A Crossover, Randomized, Double-Blind Clinical Trial

 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Results
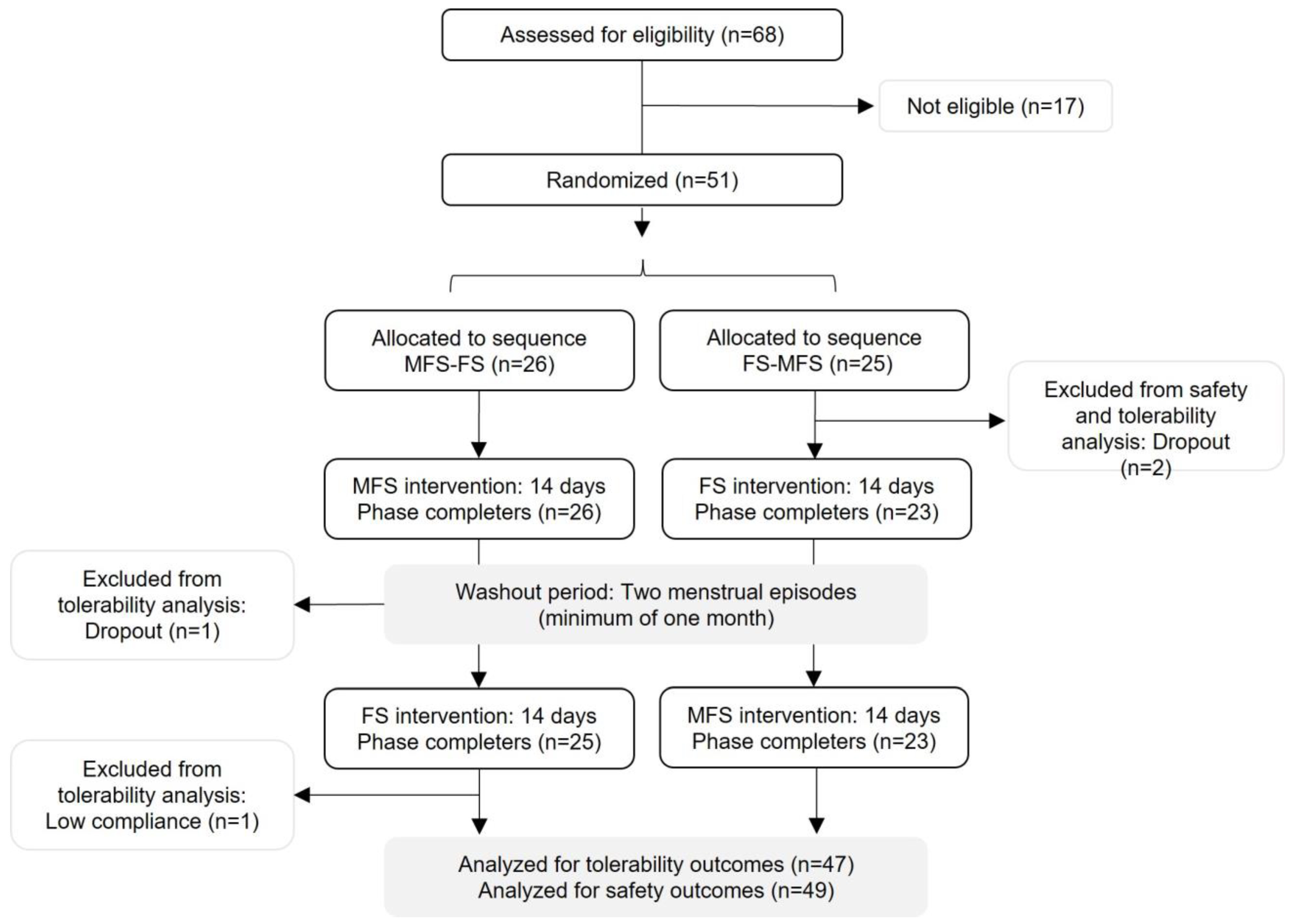
2.1. Study Population and Compliance
2.2. Primary Outcome
2.3. Secondary Outcomes
2.3.1. Frequency of Symptoms
2.3.2. Number of Complaints/Symptoms
2.3.3. Intensity of Symptoms
2.3.4. Duration of Symptoms
2.3.5. Health Status, Daily Activity, Bowel Movement, Stool Consistency
2.3.6. Sleep Duration and Quality
2.3.7. Iron Parameters
2.4. Safety Evaluation
3. Discussion
4. Materials and Methods
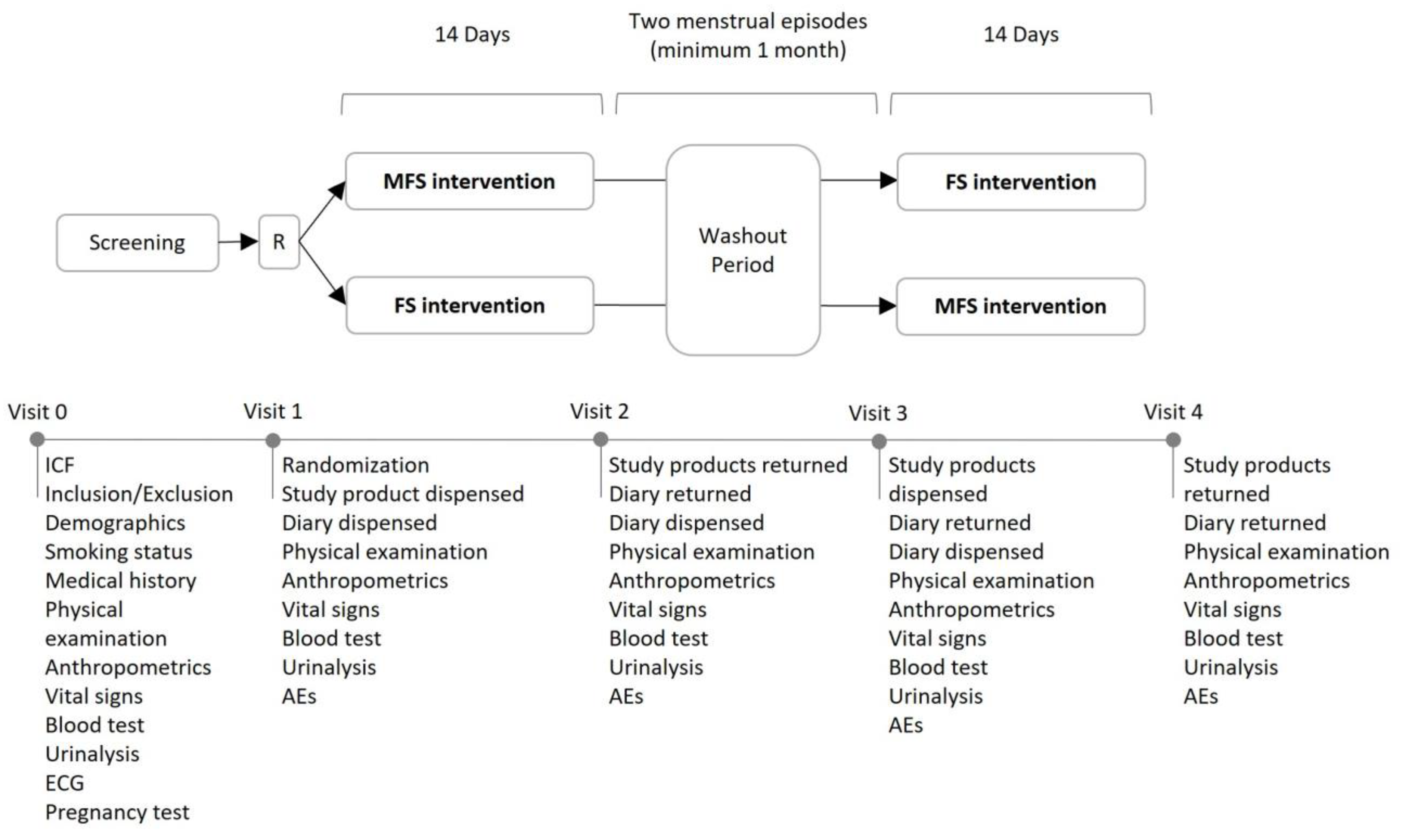
4.1. Study Design
4.2. Participants
4.3. Study Protocol and Data Collection
4.4. Study Products
4.5. Randomization and Blinding
4.6. Outcomes
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Conrad, M.E.; Umbreit, J.N. Iron Absorption: Relative Importance of Iron Transport Pathways. Am. J. Hematol. 2001, 67, 215. [Google Scholar] [CrossRef]
- Galaris, D.; Barbouti, A.; Pantopoulos, K. Iron Homeostasis and Oxidative Stress: An Intimate Relationship. Biochim. Biophys. Acta Mol. Cell Res. 2019, 1866, 118535. [Google Scholar] [CrossRef]
- Abbaspour, N.; Hurrell, R.; Kelishadi, R. Review on Iron and Its Importance for Human Health. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2014, 19, 164. [Google Scholar]
- Camaschella, C. Iron Deficiency. Blood 2019, 133, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, L.J.; Armah, C.N.; Dainty, J.R.; Foxall, R.J.; Lewis, D.J.; Langford, N.J.; Fairweather-Tait, S.J. Impact of Menstrual Blood Loss and Diet on Iron Deficiency among Women in the UK. Br. J. Nutr. 2005, 94, 557–564. [Google Scholar] [CrossRef] [Green Version]
- Milman, N.T. Dietary Iron Intake in Women of Reproductive Age in Europe: A Review of 49 Studies from 29 Countries in the Period 1993–2015. J. Nutr. Metab. 2019, 2019, 7631306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Lourdes Samaniego-Vaesken, M.; Partearroyo, T.; Olza, J.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Iron Intake and Dietary Sources in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9, 203. [Google Scholar] [CrossRef] [Green Version]
- Delimont, N.M.; Haub, M.D.; Lindshield, B.L. The Impact of Tannin Consumption on Iron Bioavailability and Status: A Narrative Review. Curr. Dev. Nutr. 2017, 1, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Hurrell, R.; Egli, I. Iron Bioavailability and Dietary Reference Values. Am. J. Clin. Nutr. 2010, 91, 1461S–1467S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Anaemia. Available online: https://www.who.int/health-topics/anaemia#tab=tab_1 (accessed on 2 August 2022).
- Miller, J.L. Iron Deficiency Anemia: A Common and Curable Disease. Cold Spring Harb. Perspect. Med. 2013, 3, a011866. [Google Scholar] [CrossRef] [Green Version]
- Skolmowska, D.; Głąbska, D. Analysis of Heme and Non-Heme Iron Intake and Iron Dietary Sources in Adolescent Menstruating Females in a National Polish Sample. Nutrients 2019, 11, 1049. [Google Scholar] [CrossRef] [PubMed]
- Casgrain, A.; Collings, R.; Harvey, L.J.; Hooper, L.; Fairweather-Tait, S.J. Effect of Iron Intake on Iron Status: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Clin. Nutr. 2012, 96, 768–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gera, T.; Sachdev, H.S.; Boy, E. Effect of Iron-Fortified Foods on Hematologic and Biological Outcomes: Systematic Review of Randomized Controlled Trials. Am. J. Clin. Nutr. 2012, 96, 309–324. [Google Scholar] [CrossRef] [Green Version]
- Man, Y.; Xu, T.; Adhikari, B.; Zhou, C.; Wang, Y.; Wang, B. Iron Supplementation and Iron-Fortified Foods: A Review. Crit. Rev. Food Sci. Nutr. 2022, 62, 4504–4525. [Google Scholar] [CrossRef]
- World Health Organization. Guideline: Iron Supplementation in Postpartum Women. Available online: http://apps.who.int/iris/handle/10665/249242 (accessed on 2 August 2022).
- Tolkien, Z.; Stecher, L.; Mander, A.P.; Pereira, D.I.A.; Powell, J.J. Ferrous Sulfate Supplementation Causes Significant Gastrointestinal Side-Effects in Adults: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0117383. [Google Scholar] [CrossRef] [Green Version]
- Cancelo-Hidalgo, M.J.; Castelo-Branco, C.; Palacios, S.; Haya-Palazuelos, J.; Ciria-Recasens, M.; Manasanch, J.; Pérez-Edo, L. Tolerability of Different Oral Iron Supplements: A Systematic Review. Curr. Med. Res. Opin. 2013, 29, 291–303. [Google Scholar] [CrossRef]
- Bouzari, Z.; Basirat, Z.; Zeinal Zadeh, M.; Cherati, S.; Ardebil, M.; Mohammadnetaj, M.; Barat, S. Daily versus Intermittent Iron Supplementation in Pregnant Women. BMC Res. Notes 2011, 4, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Mukhopadhyay, A.; Bhatla, N.; Kriplani, A.; Pandey, R.M.; Saxena, R. Daily versus Intermittent Iron Supplementation in Pregnant Women: Hematological and Pregnancy Outcome. J. Obstet. Gynaecol. Res. 2004, 30, 409–417. [Google Scholar] [CrossRef]
- Stoffel, N.U.; von Siebenthal, H.K.; Moretti, D.; Zimmermann, M.B. Oral Iron Supplementation in Iron-Deficient Women: How Much and How Often? Mol. Aspects Med. 2020, 75, 100865. [Google Scholar] [CrossRef]
- de Souza, A.I.; Filho, M.B.; Bresani, C.C.; Ferreira, L.O.C.; Figueiroa, J.N. Adherence and Side Effects of Three Ferrous Sulfate Treatment Regimens on Anemic Pregnant Women in Clinical Trials. Cad. de Saude Publica 2009, 25, 1225–1233. [Google Scholar] [CrossRef] [Green Version]
- Bloor, S.R.; Schutte, R.; Hobson, A.R. Oral Iron Supplementation—Gastrointestinal Side Effects and the Impact on the Gut Microbiota. Microbiol. Res. 2021, 12, 491–502. [Google Scholar] [CrossRef]
- Abbasi, S.; Azari, S. Efficiency of Novel Iron Microencapsulation Techniques: Fortification of Milk. Int. J. Food Sci. Technol. 2011, 46, 1927–1933. [Google Scholar] [CrossRef]
- Bryszewska, M.A. Comparison Study of Iron Bioaccessibility from Dietary Supplements and Microencapsulated Preparations. Nutrients 2019, 11, 273. [Google Scholar] [CrossRef] [Green Version]
- Hurrell, R.F. Fortification: Overcoming Technical and Practical Barriers. J. Nutr. 2002, 132, 806S–812S. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Guidelines on Food Fortification with Micronutrients. Available online: https://apps.who.int/iris/handle/10665/43412 (accessed on 2 August 2022).
- Nguyen, M.; Tadi, P. Iron Supplementation; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Peyrin-Biroulet, L.; Williet, N.; Cacoub, P. Guidelines on the Diagnosis and Treatment of Iron Deficiency across Indications: A Systematic Review. Am. J. Clin. Nutr. 2015, 102, 1585–1594. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, M.B.; Hurrell, R.F. Nutritional Iron Deficiency. Lancet 2007, 370, 511–520. [Google Scholar] [CrossRef]
- Mims, M.P.; Prchal, J.T. Divalent Metal Transporter 1. Hematology 2005, 10, 339–345. [Google Scholar] [CrossRef]
- Yanatori, I.; Kishi, F. DMT1 and Iron Transport. Free Radic. Biol. Med. 2019, 133, 55–63. [Google Scholar] [CrossRef]
- Qi, X.; Zhang, Y.; Guo, H.; Hai, Y.; Luo, Y.; Yue, T. Mechanism and Intervention Measures of Iron Side Effects on the Intestine. Crit. Rev. Food Sci. Nutr. 2020, 60, 2113–2125. [Google Scholar] [CrossRef]
- Lázaro, E.; Santas, J.; Rafecas, M. Recovery from Dietary Iron Deficiency Anaemia in Rats by the Intake of Microencapsulated Ferric Saccharate. J. Food Sci. Technol. 2017, 54, 2913–2918. [Google Scholar] [CrossRef]
- Contreras, C.; Barnuevo, M.D.; Guillén, I.; Luque, A.; Lázaro, E.; Espadaler, J.; López-Román, J.; Villegas, J.A. Comparative Study of the Oral Absorption of Microencapsulated Ferric Saccharate and Ferrous Sulfate in Humans. Eur. J. Nutr. 2014, 53, 567–574. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Daily Iron Supplementation in Adult Women and Adolescent Girls. Available online: https://apps.who.int/iris/handle/10665/204761 (accessed on 2 August 2022).
- Pereira, D.I.A.; Couto Irving, S.S.; Lomer, M.C.E.; Powell, J.J. A Rapid, Simple Questionnaire to Assess Gastrointestinal Symptoms after Oral Ferrous Sulphate Supplementation. BMC Gastroenterol. 2014, 14, 103. [Google Scholar] [CrossRef] [Green Version]
- Guideline ICH Harmonised. Integrated Addendum to ICH E6 (R1): Guideline for Good Clinical Practice E6 (R2). Curr. Step 2015, 2, 1–60. [Google Scholar]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Lewis, S.J.; Heaton, K.W. Stool Form Scale as a Useful Guide to Intestinal Transit Time. Scand. J. Gastroenterol. 1997, 32, 920–924. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total (n = 47) | Sequence | |
|---|---|---|---|
| MFS-FS (n = 24) | FS-MFS (n = 23) | ||
| Age (years) | 30.7 (7.4) | 30.6 (6.9) | 30.8 (8.1) |
| Ethnicity, n (%) | |||
| Caucasian | 47 (100.0) | 24 (100.0) | 23 (100.0) |
| BMI (kg/m2) | 22.3 (1.8) | 22.3 (1.7) | 22.4 (1.9) |
| Heart rate (beats/min) | 73.0 (12.9) | 72.1 (14.6) | 74.0 (11.2) |
| SBP (mmHg) | 114.5 (12.0) | 111.5 (10.3) | 117.5 (13.2) |
| DBP (mmHg) | 70.5 (7.6) | 70.8 (7.3) | 70.3 (8.1) |
| Current smokers, n (%) | 10 (21.3) | 6 (25.0) | 4 (17.4) |
| Ferritin level > 30 µg/L, n (%) | 19 (40.4) | 9 (37.5) | 10 (43.5) |
| Hemoglobin (g/dL) | 13.3 (0.8) | 13.1 (0.7) | 13.5 (0.7) |
| Ferritin level (µg/L) | 30.5 (19.6) | 27.8 (15.6) | 33.3 (23.1) |
| Transferrin saturation (%) | 28.6 (11.9) | 27.2 (12.8) | 30.0 (11.0) |
| Serum iron (µg/dL) | 93.0 (36.6) | 86.3 (38.1) | 100.0 (95.1) |
| Participants | Study Period | p Values * | ||||
|---|---|---|---|---|---|---|
| MFS | FS | Washout | P1 | P2 | P3 | |
| Symptoms experienced | 34 (72.3) | 43 (91.5) | 35 (74.5) | 0.012 | 1.000 | 0.039 |
| No symptoms experienced | 13 (27.7) | 4 (8.5) | 12 (25.5) | |||
| Symptoms | Study Period | p Values * | ||||
|---|---|---|---|---|---|---|
| MFS (n = 47) | FS (n = 47) | Washout (n = 47) | P1 | P2 | P3 | |
| GI-related symptoms | 32 (68.1) | 41 (87.2) | 30 (63.8) | 0.012 | 0.774 | 0.003 |
| Nausea | 4 (8.5) | 11 (23.4) | 2 (4.3) | 0.016 | 0.687 | 0.022 |
| Heartburn | 7 (14.9) | 10 (21.3) | 3 (6.4) | 0.508 | 0.219 | 0.039 |
| Abdominal pain | 10 (21.3) | 17 (36.2) | 15 (31.9) | 0.039 | 0.302 | 0.815 |
| Flatulence/swelling | 20 (42.6) | 30 (63.8) | 19 (40.4) | 0.013 | 1.000 | 0.007 |
| Diarrhea | 6 (12.8) | 14 (29.8) | 5 (10.6) | 0.039 | 1.000 | 0.012 |
| Metallic taste | 3 (6.4) | 6 (12.8) | 1 (2.1) | 0.375 | 0.500 | 0.063 |
| Constipation | 11 (23.4) | 12 (25.5) | 9 (19.1) | 1.000 | 0.804 | 0.629 |
| Vomiting | 0 (0.0) | 1 (2.1) | 0 (0.0) | 1.000 | NA | 1.000 |
| Headache | 17 (36.2) | 24 (51.1) | 20 (42.6) | 0.143 | 0.664 | 0.523 |
| Shortness of breath | 1 (2.1) | 2 (4.3) | 0 (0.0) | 1.000 | 1.000 | 0.500 |
| Reports | Subjects † | Study Period | p Values * | ||||
|---|---|---|---|---|---|---|---|
| MFS | FS | Washout | P1 | P2 | P3 | ||
| Number of complaints | |||||||
| Total | 45 | 4.6 (5.1) | 8.8 (8.1) | 3.5 (3.7) | <0.001 | 0.169 | <0.001 |
| GI-related | 42 | 4.0 (4.3) | 7.7 (6.7) | 2.8 (3.4) | 0.001 | 0.105 | <0.001 |
| Number of symptoms | |||||||
| Total | 45 | 1.8 (1.5) | 2.8 (1.7) | 1.6 (1.3) | <0.001 | 0.646 | <0.001 |
| GI-related | 42 | 1.5 (1.2) | 2.4 (1.4) | 1.3 (1.1) | <0.001 | 0.426 | <0.001 |
| Symptoms | Subjects † | Study Period | p Values * | ||||
|---|---|---|---|---|---|---|---|
| MFS | FS | Washout | P1 | P2 | P3 | ||
| Nausea (cm) | 13 | 0.8 (1.6) | 3.4 (2.6) | 0.6 (1.5) | 0.006 | 0.752 | 0.039 |
| Heartburn (cm) | 13 | 1.2 (1.4) | 2.1 (2.5) | 0.5 (1.1) | 0.507 | 0.017 | 0.062 |
| Abdominal pain (cm) | 26 | 1.6 (2.5) | 3.0 (2.9) | 2.7 (2.6) | 0.010 | 0.179 | 0.677 |
| Flatulence/swelling (cm) | 34 | 2.2 (2.5) | 3.1 (2.6) | 2.1 (2.5) | <0.002 | 0.785 | 0.037 |
| Diarrhea (events/day) | 17 | 1.0 (1.6) | 2.0 (1.2) | 1.1 (1.9) | 0.122 | 1.000 | 0.052 |
| Vomiting (events/day) | 1 | 0.0 (0.0) | 2.5 (0.0) | 0.0 (0.0) | NA | NA | NA |
| Symptoms | Subjects † | Study Period | p Values * | ||||
|---|---|---|---|---|---|---|---|
| MFS (days) | FS (days) | Washout (days) | P1 | P2 | P3 | ||
| Nausea | 13 | 0.3 (0.5) | 2.2 (2.2) | 0.1 (0.4) | 0.005 | 0.414 | 0.008 |
| Heartburn | 13 | 1.4 (1.7) | 1.5 (1.4) | 0.5 (1.1) | 0.843 | 0.065 | 0.051 |
| Abdominal pain | 26 | 0.8 (1.2) | 1.7 (2.2) | 1.0 (1.1) | 0.017 | 0.552 | 0.208 |
| Flatulence/swelling | 34 | 2.3 (3.4) | 3.9 (3.6) | 1.6 (2.7) | 0.008 | 0.174 | <0.001 |
| Diarrhea | 17 | 0.7 (1.2) | 1.6 (1.3) | 0.4 (0.8) | 0.025 | 0.160 | 0.003 |
| Metallic taste | 7 | 0.4 (0.5) | 4.0 (4.1) | 0.1 (0.4) | 0.058 | 0.157 | 0.042 |
| Constipation | 25 | 1.3 (1.8) | 1.5 (2.0) | 1.0 (1.7) | 0.924 | 0.569 | 0.419 |
| Vomiting | 1 | 0.0 (0.0) | 2.0 (0.0) | 0.0 (0.0) | NA | NA | NA |
| Headache | 36 | 1.1 (1.7) | 1.9 (2.9) | 1.1 (1.3) | 0.101 | 0.876 | 0.198 |
| Shortness of breath | 3 | 0.3 (0.6) | 0.7 (0.6) | 0.0 (0.0) | 0.564 | 0.317 | 0.147 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Friling, M.; García-Muñoz, A.M.; Perrinjaquet-Moccetti, T.; Victoria-Montesinos, D.; Pérez-Piñero, S.; Abellán-Ruiz, M.S.; Luque-Rubia, A.J.; García-Guillén, A.I.; Cánovas, F.; Ivanir, E. Tolerability of Oral Supplementation with Microencapsulated Ferric Saccharate Compared to Ferrous Sulphate in Healthy Premenopausal Woman: A Crossover, Randomized, Double-Blind Clinical Trial. Int. J. Mol. Sci. 2022, 23, 12282. https://doi.org/10.3390/ijms232012282
Friling M, García-Muñoz AM, Perrinjaquet-Moccetti T, Victoria-Montesinos D, Pérez-Piñero S, Abellán-Ruiz MS, Luque-Rubia AJ, García-Guillén AI, Cánovas F, Ivanir E. Tolerability of Oral Supplementation with Microencapsulated Ferric Saccharate Compared to Ferrous Sulphate in Healthy Premenopausal Woman: A Crossover, Randomized, Double-Blind Clinical Trial. International Journal of Molecular Sciences. 2022; 23(20):12282. https://doi.org/10.3390/ijms232012282
Chicago/Turabian StyleFriling, Marina, Ana María García-Muñoz, Tania Perrinjaquet-Moccetti, Desirée Victoria-Montesinos, Silvia Pérez-Piñero, María Salud Abellán-Ruiz, Antonio J. Luque-Rubia, Ana Isabel García-Guillén, Fernando Cánovas, and Eran Ivanir. 2022. "Tolerability of Oral Supplementation with Microencapsulated Ferric Saccharate Compared to Ferrous Sulphate in Healthy Premenopausal Woman: A Crossover, Randomized, Double-Blind Clinical Trial" International Journal of Molecular Sciences 23, no. 20: 12282. https://doi.org/10.3390/ijms232012282