
Exploring the Association between Welfare State and Mental Wellbeing in Europe: Does Age Matter?
 , , , and
, , , and
Abstract
:1. Introduction
1.1. Age, Mental Wellbeing, and the Welfare State
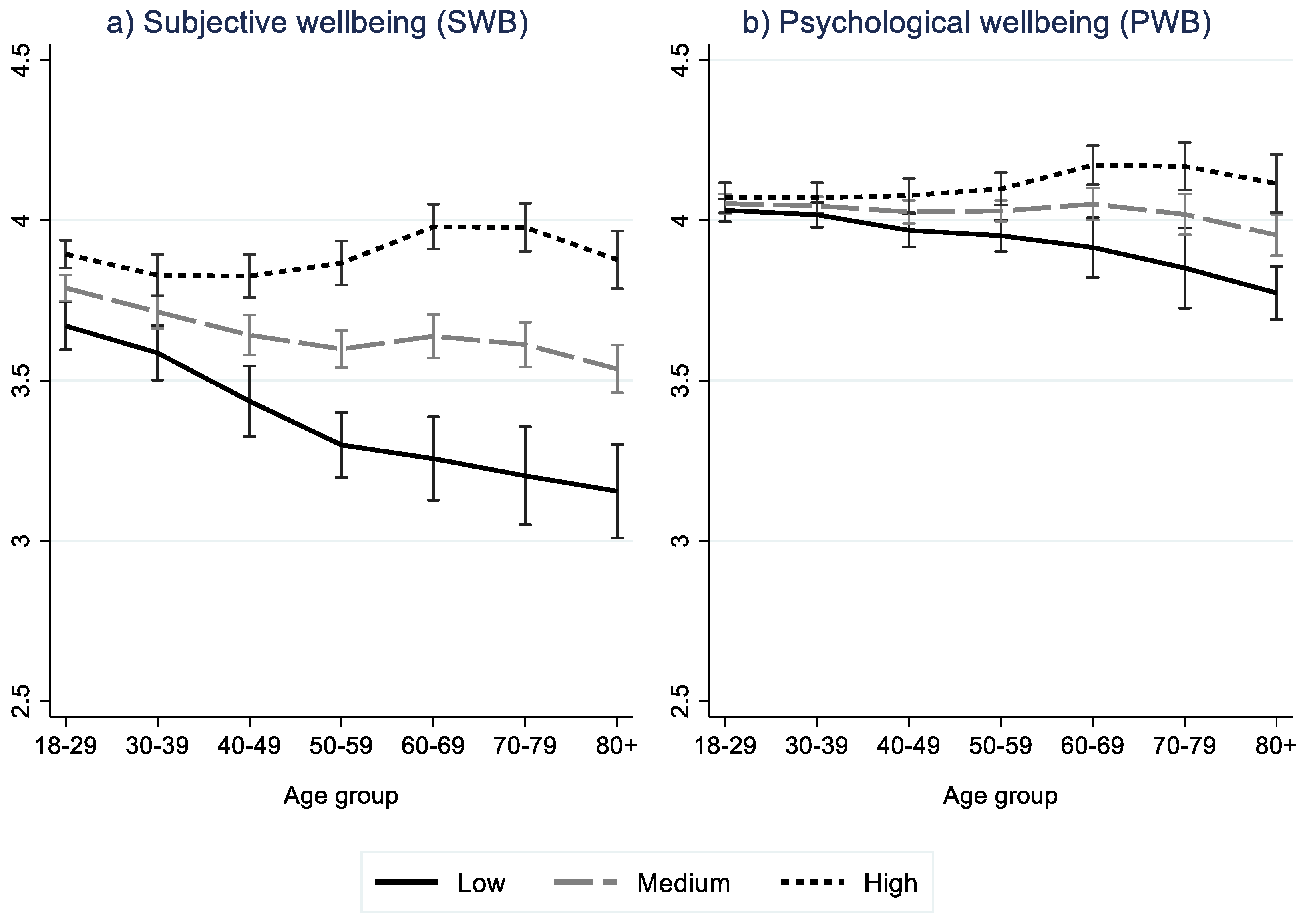
1.2. Mental Wellbeing over the Life Course
1.3. Welfare State Impact on Health and Wellbeing
1.4. Study Objectives and Research Questions
- (i)
- to explore the association between MWB and WS;
- (ii)
- to explore the age gradient in the association between MWB and WS.
2. Materials and Methods
2.1. Data Materials
2.2. Measuring Mental Wellbeing
- All individual items (X) were normalized (Xnorm) using the min–max algorithm such that all items take on values in the interval 1–5:Xnorm = ((5 − 1)/(Xmax − Xmin)) × (X − Xmax) + 5
- Each of the five retained MWB factors from the original ESEM analysis were calculated as means of the normalized items included. See Table A3 for an overview of items included in each of the five factors.
- SWB was measured as the mean of “evaluative wellbeing” and “emotional wellbeing” factors, whereas PWB was measured as the mean of “positive psychological functioning”, “flow”, and “positive relationships” factors.
2.3. Welfare State Measures
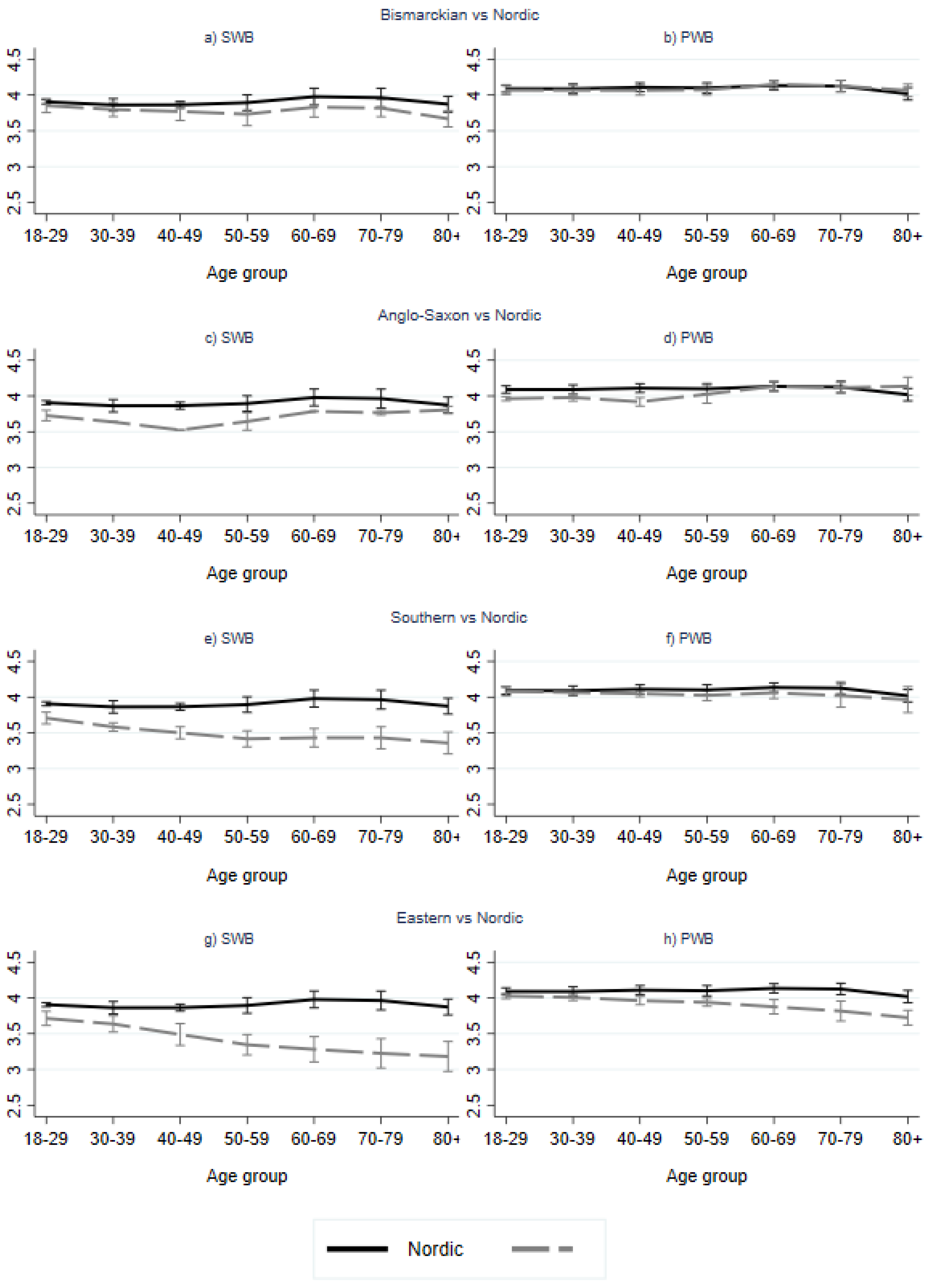
2.3.1. Regime Typology (Dummy Variable Approach)
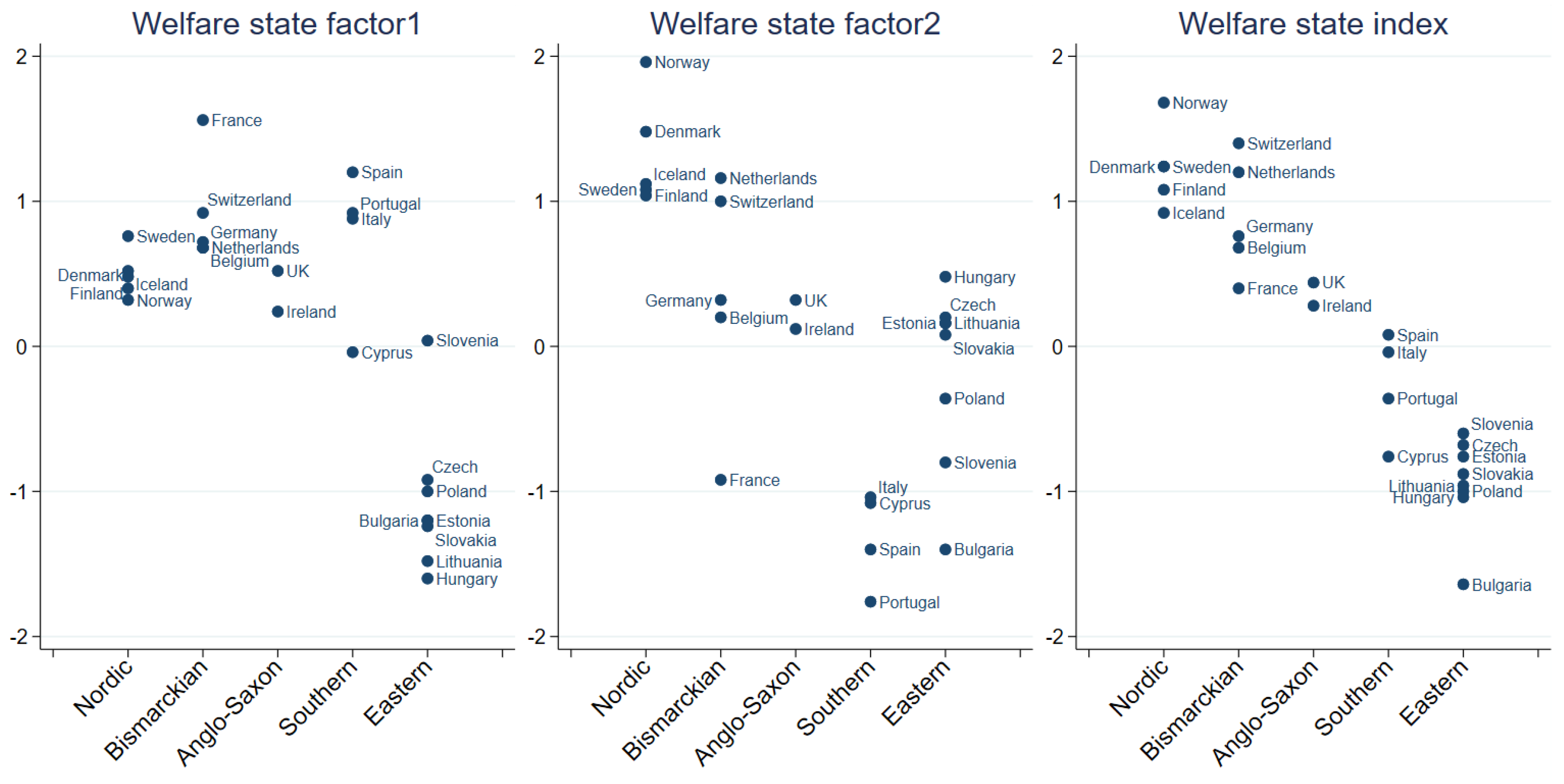
2.3.2. Welfare State Index
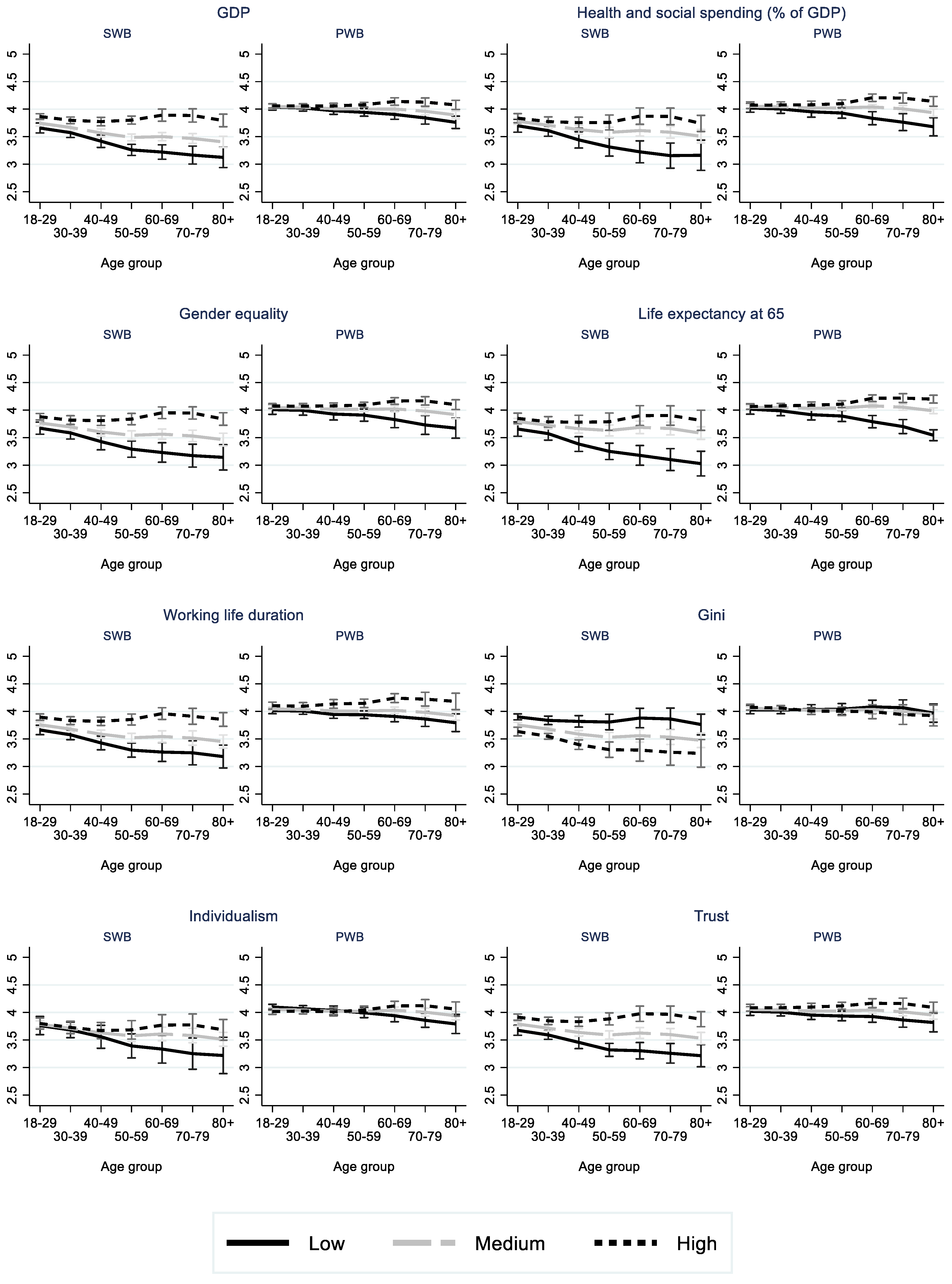
2.3.3. Welfare State Factors
2.4. Statistical Analyses
3. Results
3.1. Values of WS Index and WS Factors by WS Regime Types
3.2. Descriptive Statistics
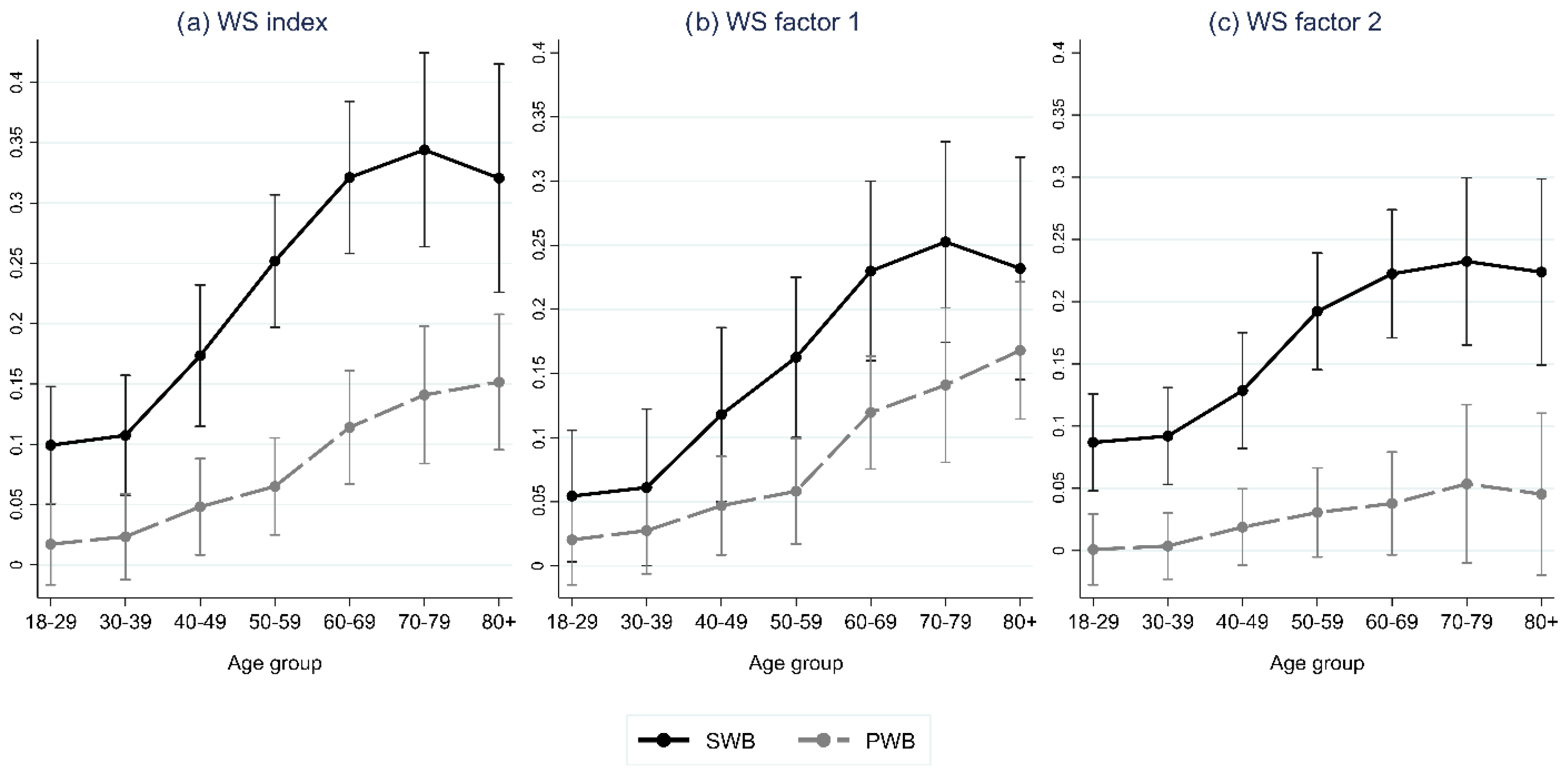
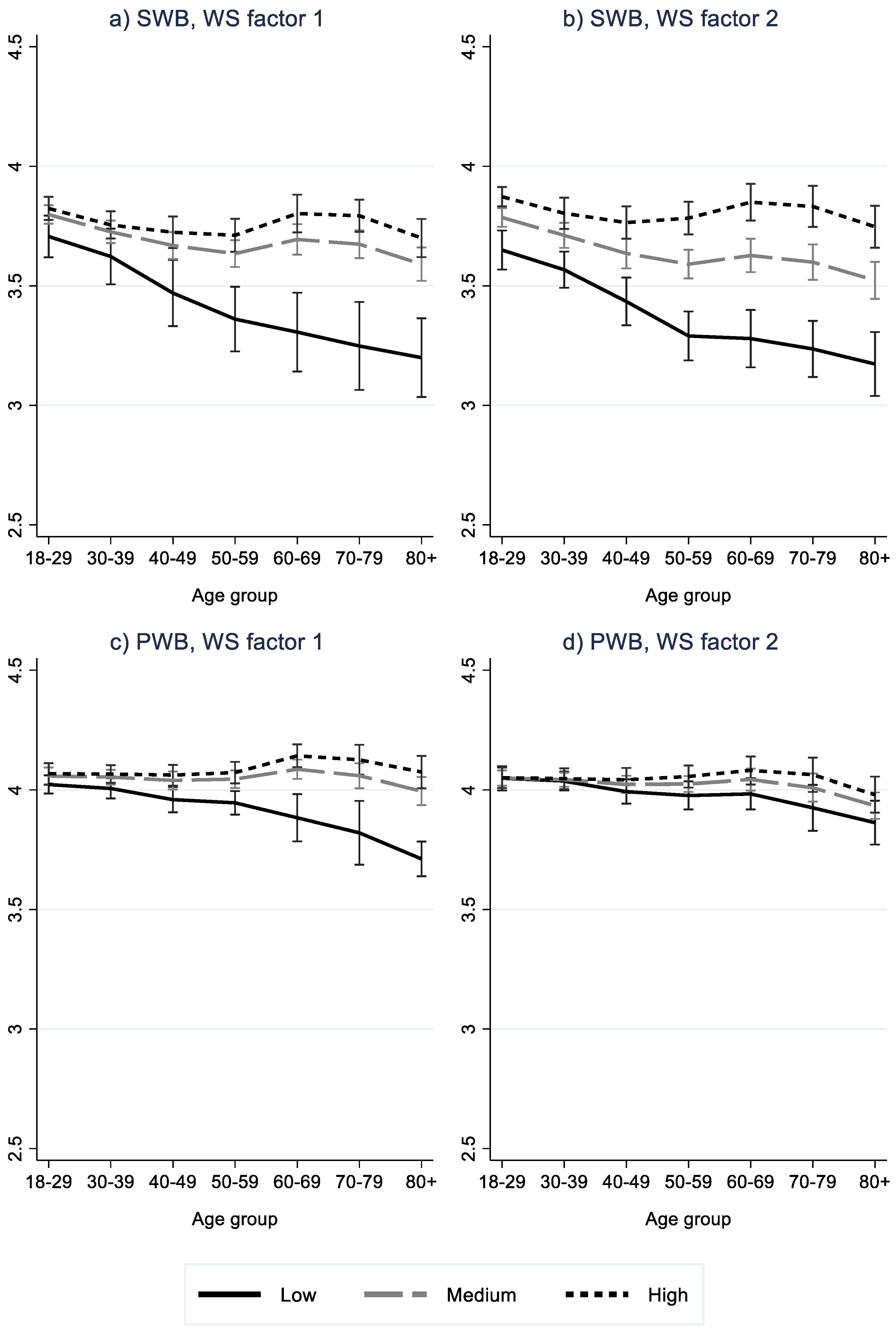
3.3. Multivariate Regression Results
4. Discussion
4.1. The Association between Welfare State and Mental Wellbeing
4.2. The Age Gradient in the Association between Welfare State and Mental Wellbeing
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Welfare State Approaches

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Regime | Population Coverage b | Role of the Private Market c | Target Population d | Decommodification e |
|---|---|---|---|---|
| Social Democratic | Universal | Low | All citizens | High |
| Conservative | Occupational | Low | Families | Medium |
| Liberal | Selective | High | Poor | Low |
| Mediterranean | Occupational | Medium | Families | Low |
| Post-Communist | Selective | Medium | Poor | Low |
Appendix B
| Variable | Description |
|---|---|
| GDP per capita | Gross Domestic Product per capita in PPS, 2012, Index (EU28 = 100), Eurostat |
| Health/GDP + Social/GDP | Health expenditure as % of GDP, the World Bank DataBank, plus Social protection expenditure as % of GDP, 2012, Eurostat |
| Gender empowerment measure | Human Development Report 2009, United Nations (compiled by the ESS Multilevel Data Repository) |
| Life expectancy at 65 | Life expectancy in absolute value at 65 (average for male and female), 2012, Eurostat |
| Duration working life | Duration of working life, 2012, Eurostat |
| GINI | Gini coefficient of equivalized disposable income (scale from 0 to 100), EU-SILC survey, 2012, Eurostat |
| Individualism | Individualism versus Collectivism Index, from Hofstede Insights, https://www.hofstede-insights.com/product/compare-countries/ (accessed on 28 May 2019). Description: The high side of this dimension, called individualism, can be defined as a preference for a loosely knit social framework in which individuals are expected to take care of only themselves and their immediate families. Its opposite, collectivism, represents a preference for a tightly knit framework in society in which individuals can expect their relatives or members of a particular ingroup to look after them in exchange for unquestioning loyalty. A society’s position on this dimension is reflected in whether people’s self-image is defined in terms of “I” or “we”. |
| Trust | Average rating of trust by domain (trust police, trust legal system, trust political system, trust others), both sexes, all educational attainment levels, 16 years or over (rating 0–10), EU—SILC survey, 2013, Eurostat, http://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=ilc_pw03 (accessed on 28 May 2019). |
| Mental Wellbeing Factor | Items |
|---|---|
| Subjective wellbeing (SWB) | |
| Evaluative wellbeing | How satisfied with life as a whole, How happy are you |
| Positive emotional wellbeing | Enjoyed life, Were happy, Felt calm and peaceful, Had lot of energy (how often past week) |
| Psychological wellbeing (PWB) | |
| Positive functioning | Free to decide how to live my life, Feel accomplishment from what I do, Feel what I do in life is valuable and worthwhile, There are lots of things I am good at, In general feel very positive about myself, Always optimistic about my future |
| Flow | Interested in what you are doing, Absorbed in what you are doing, Enthusiastic about what you are doing |
| Positive relationships | Feel people treat you with respect, Feel appreciated by people you are close to, Provide help and support to people you are close to, Receive help and support from people you are close to |
| Variable | Restricting to One Factor | Using the Kaiser Criterion | |||
|---|---|---|---|---|---|
| Factor1 | Uniqueness | Factor1 a | Factor2 a | Uniqueness | |
| GDP per capita | 0.9191 | 0.1552 | 0.6552 | 0.6583 | 0.1374 |
| Health/GDP + Social/GDP | 0.7738 | 0.4012 | 0.9023 | 0.1834 | 0.1522 |
| Gender empowerment measure | 0.9178 | 0.1576 | 0.7611 | 0.5421 | 0.1269 |
| Life expectancy at 65 | 0.7532 | 0.4327 | 0.9568 | 0.0869 | 0.077 |
| Work life duration | 0.7285 | 0.4692 | 0.4464 | 0.6272 | 0.4073 |
| GINI | −0.5459 | 0.702 | −0.1759 | −0.6969 | 0.4834 |
| Individualism | 0.5364 | 0.7123 | 0.2092 | 0.6422 | 0.5438 |
| Trust | 0.7124 | 0.4924 | 0.1747 | 0.8928 | 0.1723 |
| WS-Variable | SWB | PWB |
|---|---|---|
| WS index | 0.72/0.72 | 0.34/0.34 |
| WS factors | 0.75/0.75 | 0.37/0.38 |
| WS regimes | 0.62/0.62 | 0.41/0.42 |
| GDP per capita | 0.68/0.67 | 0.28/0.28 |
| Health and social spending (% of GDP) | 0.33/0.33 | 0.25/0.26 |
| Gender equality | 0.54/0.54 | 0.27/0.28 |
| Longevity at 65 | 0.41/0.41 | 0.33/0.34 |
| Working life duration | 0.55/0.55 | 0.24/0.24 |
| Gini coefficient | 0.42/0.42 | 0.00/0.00 |
| Individualism | 0.12/0.12 | 0.01/0.01 |
| Social trust | 0.51/0.52 | 0.19/0.19 |
| WS Index | WS Factor 1 | WS Factor 2 | GDP | Health and Social Spending | Gender Equality | Life Expectancy at 65 | Working Life Duration | Gini | Individualism | Social Trust | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| WS index | 1 | ||||||||||
| WS factor 1 | 0.7555 | 1 | |||||||||
| WS factor 2 | 0.648 | 0 | 1 | ||||||||
| GDP | 0.9404 | 0.6552 | 0.6583 | 1 | |||||||
| Health and Social spending | 0.7917 | 0.9023 | 0.1834 | 0.6675 | 1 | ||||||
| Gender equality | 0.939 | 0.7611 | 0.5421 | 0.8022 | 0.7794 | 1 | |||||
| Life expectancy at 65 | 0.7706 | 0.9567 | 0.087 | 0.6986 | 0.8113 | 0.7241 | 1 | ||||
| Working life duration | 0.7454 | 0.4464 | 0.6273 | 0.6785 | 0.3657 | 0.6788 | 0.5224 | 1 | |||
| Gini | −0.559 | −0.176 | −0.697 | −0.579 | −0.339 | −0.471 | −0.239 | −0.411 | 1 | ||
| Individualism | 0.5488 | 0.2093 | 0.6421 | 0.5102 | 0.3886 | 0.5168 | 0.2411 | 0.2638 | −0.297 | 1 | |
| Social trust | 0.7289 | 0.1747 | 0.8928 | 0.6915 | 0.3406 | 0.6112 | 0.2461 | 0.6484 | −0.493 | 0.544 | 1 |

References
- European Commission. The 2021 Ageing Report. Underlying Assumptions and Projection Methodologies; European Economy, Institutional Paper 142; European Commission: Brussels, Belgium, 2020. [Google Scholar]
- Steptoe, A.; Deaton, A.; Stone, A.A. Subjective wellbeing, health, and ageing. Lancet 2015, 385, 640–648. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- World Health Organization. Global Strategy and Action Plan on Ageing and Health; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Kaufmann, F.-X. Major Problems and Dimensions of the Welfare State; Croom Helm: London, UK, 1985. [Google Scholar]
- Marmot, M.; Wilkinson, R. Social Determinants of Health; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- World Health Organization. Promoting Mental Health: Concepts, Emerging Evidence, Practice: Summary Report; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Keyes, C.L.M. Promoting and protecting mental health as flourishing: A complementary strategy for improving national mental health. Am. Psychol. 2007, 62, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L. Chronic physical conditions and aging: Is mental health a potential protective factor? Ageing Int. 2005, 30, 88–104. [Google Scholar] [CrossRef]
- Lara, E.; Martín-María, N.; Forsman, A.K.; Cresswell-Smith, J.; Donisi, V.; Ådnanes, M.; Kaasbøll, J.; Melby, L.; Nordmyr, J.; Nyholm, L.; et al. Understanding the multi-dimensional mental well-being in late life: Evidence from the perspective of the oldest old population. J. Happiness Stud. 2020, 21, 465–484. [Google Scholar] [CrossRef]
- Cresswell-Smith, J.; Amaddeo, F.; Donisi, V.; Forsman, A.K.; Kalseth, J.; Martin-Maria, N.; Miret, M.; Walhbeck, K. Determinants of multidimensional mental wellbeing in the oldest old: A rapid review. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 135–144. [Google Scholar] [CrossRef]
- Diener, E.; Suh, E.M.; Lucas, R.E.; Smith, H.L. Subjective well-being: Three decades of progress. Psychol. Bull. 1999, 125, 276. [Google Scholar] [CrossRef]
- Ryff, C.D. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Personal. Soc. Psychol. 1989, 57, 1069. [Google Scholar] [CrossRef]
- Ryff, C.D.; Singer, B.H. Know Thyself and Become What You Are: A Eudaimonic Approach to Psychological Well-Being. J. Happiness Stud. 2008, 9, 13–39. [Google Scholar] [CrossRef]
- Ulloa, B.F.L.; Møller, V.; Sousa-Poza, A. How Does Subjective Well-Being Evolve with Age? A Literature Review. J. Popul. Ageing 2013, 6, 227–246. [Google Scholar] [CrossRef]
- Golden, J.; Conroy, R.M.; Bruce, I.; Denihan, A.; Greene, E.; Kirby, M.; Lawlor, B.A. Loneliness, social support networks, mood and wellbeing in community-dwelling elderly. Int. J. Geriatr. Psychiatry 2009, 24, 694–700. [Google Scholar] [CrossRef]
- Nyqvist, F.; Forsman, A.K.; Cattan, M. A comparison of older workers’ and retired older people’s social capital and sense of mastery. Scand. J. Public Health 2013, 41, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Schwandt, H. Unmet aspirations as an explanation for the age U-shape in wellbeing. J. Econ. Behav. Organ. 2016, 122, 75–87. [Google Scholar] [CrossRef]
- Cheng, T.C.; Powdthavee, N.; Oswald, A.J. Longitudinal Evidence for a Midlife Nadir in Human Well-Being: Results from Four Data Sets. Econ. J. 2015, 127, 126–142. [Google Scholar] [CrossRef] [PubMed]
- Carstensen, L.L.; Fung, H.H.-L.; Charles, S.T. Socioemotional Selectivity Theory and the Regulation of Emotion in the Second Half of Life. Motiv. Emot. 2003, 27, 103–123. [Google Scholar] [CrossRef]
- Forsman, A.K.; Herberts, C.; Nyqvist, F.; Wahlbeck, K.; Schierenbeck, I. Understanding the role of social capital for mental wellbeing among older adults. Ageing Soc. 2012, 33, 804–825. [Google Scholar] [CrossRef]
- Alesina, A.; Di Tella, R.; MacCulloch, R. Inequality and happiness: Are Europeans and Americans different? J. Public Econ. 2004, 88, 2009–2042. [Google Scholar] [CrossRef]
- Muntaner, C.; Borrell, C.; Ng, E.; Chung, H.; Espelt, A.; Rodriguez-Sanz, M.; Benach, J.; O’Campo, P. Politics, welfare regimes, and population health: Controversies and evidence. Sociol. Health Illn. 2011, 33, 946–964. [Google Scholar] [CrossRef]
- Pedersen, A.W.; Kuhnle, S. The Nordic welfare state model. In The Nordic Models in Political Science. Challenged, but Still Viable? Fagbokforlaget: Bergen, Norway, 2017. [Google Scholar]
- Eikemo, T.A.; Bambra, C.; Judge, K.; Ringdal, K. Welfare state regimes and differences in self-perceived health in Europe: A multilevel analysis. Soc. Sci. Med. 2008, 66, 2281–2295. [Google Scholar] [CrossRef]
- Richter, M.; Rathman, K.; Nic Gabhainn, S.; Zambon, A.; Boyce, W.; Hurrelmann, K. Welfare state regimes, health and health inequalities in adolescence: A multilevel study in 32 countries. Sociol. Health Illn. 2012, 34, 858–879. [Google Scholar] [CrossRef]
- Chung, H.; Muntaner, C. Welfare state matters: A typological multilevel analysis of wealthy countries. Health Policy 2006, 80, 328–339. [Google Scholar] [CrossRef]
- Guarnizo-Herreño, C.C.; Tsakos, G.; Sheiham, A.; Watt, R. Oral health and welfare state regimes: A cross-national analysis of European countries. Eur. J. Oral Sci. 2013, 121, 169–175. [Google Scholar] [CrossRef]
- Kim, I.H.; Muntaner, C.; Shahidi, F.V.; Vives, A.; Vanroelen, C.; Benach, J. Welfare states, flexible employment, and health: A critical review. Health Policy 2012, 104, 99–127. [Google Scholar] [CrossRef] [PubMed]
- Deeming, C.; Hayes, D. Worlds of Welfare Capitalism and Wellbeing: A Multilevel Analysis. J. Soc. Policy 2012, 41, 811–829. [Google Scholar] [CrossRef]
- Ejrnæs, A.; Greve, B. Your position in society matters for how happy you are. Int. J. Soc. Welf. 2016, 26, 206–217. [Google Scholar] [CrossRef]
- Rothstein, B. Happiness and the welfare state. Soc. Res. 2010, 77, 441–468. [Google Scholar] [CrossRef]
- Deeming, C.; Jones, K. Investigating the Macro Determinants of Self-Rated Health and Well-Being Using the European Social Survey: Methodological Innovations across Countries and Time. Int. J. Sociol. 2015, 45, 256–285. [Google Scholar] [CrossRef]
- Barr, N.A. The Welfare State as Piggy Bank: Information, Risk, Uncertainty, and the Role of the State; Oxford University Press: Oxford, UK, 2001. [Google Scholar]
- European Social Survey. ESS Round 6: European Social Survey Round 6 Data (2012); Data File Edition 2.4. NSD—Norwegian Centre for Research Data, Norway—Data Archive and Distributor of ESS Data for ESS ERIC; European Social Survey: London, UK, 2012. [Google Scholar] [CrossRef]
- Donisi, V.; Tedeschi, F.; Gonzalez-Caballero, J.L.; Cresswell-Smith, J.; Lara, E.; Miret, M.; Forsman, A.K.; Wahlbeck, K.; Amaddeo, F.; Kalseth, J. Is Mental Well-Being in the Oldest Old Different from That in Younger Age Groups? Exploring the Mental Well-Being of the Oldest-Old Population in Europe. J. Happiness Stud. 2020, 22, 1693–1717. [Google Scholar] [CrossRef]
- Seligman, M.E.P. Flourish; Simon & Schuster: New York, NY, USA, 2011. [Google Scholar]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh mental well-being scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Joshanloo, M.; Sirgy, M.J.; Park, J. Directionality of the relationship between social well-being and subjective well-being: Evidence from a 20-year longitudinal study. Qual. Life Res. 2018, 27, 2137–2145. [Google Scholar] [CrossRef]
- Keyes, C.L.M. The Mental Health Continuum: From Languishing to Flourishing in Life. J. Health Soc. Behav. 2002, 43, 207–222. [Google Scholar] [CrossRef]
- Esping Andersen, G. The Three Worlds of Welfare Capitalism; Princeton University Press: Princeton, NJ, USA, 1990. [Google Scholar]
- Rice, D. Beyond Welfare Regimes: From Empirical Typology to Conceptual Ideal types. Soc. Policy Adm. 2012, 47, 93–110. [Google Scholar] [CrossRef]
- Huber, E.; Stephens, J.D.; Bradley, D.; Moller, S.; Nielsen, F. The Welfare State and Gender Equality; LIS Working Paper Series; Luxembourg Income Study (LIS): Luxembourg, 2001. [Google Scholar]
- Arts, W.; Gelissen, J. Three worlds of welfare capitalism or more? A state-of-the-art report. J. Eur. Soc. Policy 2002, 12, 137–158. [Google Scholar] [CrossRef]
- Bambra, C. Going beyond the three worlds of welfare capitalism: Regime theory and public health research. J. Epidemiol. Community Health 2007, 61, 1098–1102. [Google Scholar] [CrossRef]
- Jorm, A.F.; Ryan, S.M. Cross-national and historical differences in subjective well-being. Int. J. Epidemiol. 2014, 43, 330–340. [Google Scholar] [CrossRef]
- European Social Survey. Weighting European Social Survey Data; Norwegian Social Science Data Services: Bergen, Norway, 2014. [Google Scholar]
- Bryk, A.S.; Raudenbush, S.W. Hierarchical Linear Models: Applications and Data Analysis Methods; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1992. [Google Scholar]
- Snijders, T.A.; Bosker, R.J. Multilevel Analysis: An Introduction to Basic and Advanced Multilevel Modeling; Sage: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Moor, N.; de Graaf, P.M.; Komter, A. Family, welfare state generosity and the vulnerability of older adults: A cross-national study. J. Aging Stud. 2013, 27, 347–357. [Google Scholar] [CrossRef]
- Pacek, A.; Radcliff, B. Assessing the Welfare State: The Politics of Happiness. Perspect. Politics 2008, 6, 267–277. [Google Scholar] [CrossRef]
- Andersen, T.M. The welfare state and economic performance. SOU 2015, 53, 2015. [Google Scholar]
- Clark, A.E. Born to be mild? Cohort effects don’t (fully) explain why well-being is U-shaped in age. In The Economics of Happiness; Springer: Berlin/Heidelberg, Germany, 2019; pp. 387–408. [Google Scholar]
- Horowitz, J. The Post-Communist Generation in the Former Eastern Bloc. 2010: Pew Research Center, Pew Global Attitudes Project. Available online: https://www.pewresearch.org/global/2010/01/20/the-post-communist-generation-in-the-former-eastern-bloc/ (accessed on 29 October 2020).
- Horvat, P.; Evans, G. Age, Inequality, and Reactions to Marketization in Post-Communist Central and Eastern Europe. Eur. Sociol. Rev. 2011, 27, 708–727. [Google Scholar] [CrossRef]
- Levecque, K.; Van Rossem, R.; De Boyser, K.; Van de Velde, S.; Bracke, P. Economic hardship and depression across the life course: The impact of welfare state regimes. J. Health Soc. Behav. 2011, 52, 262–276. [Google Scholar] [CrossRef]
- Vanhuysse, P.; Medgyesi, M.; Gal, R.I. Welfare states as lifecycle redistribution machines: Decomposing the roles of age and socio-economic status shows that European tax-and-benefit systems primarily redistribute across age groups. PLoS ONE 2021, 16, e0255760. [Google Scholar] [CrossRef] [PubMed]
- Chlon-Dominczak, A.; Abramowska-Kmon, A.; Kotowska, I.E.; Łątkowski, W.; Strzelecki, P.A. Welfare state and the age distribution of public consumption and public transfers in the EU countries. Vienna Yearb. Popul. Res. 2019, 1, 71–97. [Google Scholar] [CrossRef]
- Nordmyr, J.; Creswell-Smith, J.; Donisi, V.; Lara, E.; Martín-María, N.; Nyholm, L.; Forsman, A.K. Mental well-being among the oldest old: Revisiting the model of healthy ageing in a Finnish context. Int. J. Qual. Stud. Health Well-Being 2020, 15, 1734276. [Google Scholar] [CrossRef] [PubMed]
- Strauss, S.; Trommer, K. Productive Ageing Regimes in Europe: Welfare State Typologies Explaining Elderly Europeans’ Participation in Paid and Unpaid Work. J. Popul. Ageing 2017, 11, 311–328. [Google Scholar] [CrossRef]
- Damiani, G.; Farelli, V.; Anselmi, A.; Sicuro, L.; Solipaca, A.; Burgio, A.; Iezzi, D.F.; Ricciardi, W. Patterns of Long Term Care in 29 European countries: Evidence from an exploratory study. BMC Health Serv. Res. 2011, 11, 316. [Google Scholar] [CrossRef]
- Conde-Sala, J.L.; Portellano-Ortiz, C.; Calvó-Perxas, L.; Garre-Olmo, J. Quality of life in people aged 65+ in Europe: Associated factors and models of social welfare—Analysis of data from the SHARE project (Wave 5). Qual. Life Res. 2016, 26, 1059–1070. [Google Scholar] [CrossRef] [PubMed]
- Bussière, C.; Sirven, N.; Tessier, P. Does ageing alter the contribution of health to subjective well-being? Soc. Sci. Med. 2021, 268, 113456. [Google Scholar] [CrossRef]
- Kunißen, K. From Dependent to Independent Variable: A Critical Assessment of Operationalisations of ‘Welfare Stateness’ as Macro-Level Indicators in Multilevel Analyses. Soc. Indic. Res. 2018, 142, 597–616. [Google Scholar] [CrossRef]
- Gwozdz, W.; Sousa-Poza, A. Ageing, Health and Life Satisfaction of the Oldest Old: An Analysis for Germany. Soc. Indic. Res. 2010, 97, 397–417. [Google Scholar] [CrossRef]
- Bryan, M.; Jenkins, S.P. Multilevel Modelling of Country Effects: A Cautionary Tale. Eur. Sociol. Rev. 2015, 32, 3–22. [Google Scholar] [CrossRef] [Green Version]
- Kim, K. Income inequality, welfare regimes and aggregate health: Review of reviews. Int. J. Soc. Welf. 2018, 28, 31–43. [Google Scholar] [CrossRef]
- Heß, A. Happiness and the Welfare State in Times of Globalization: A review of Empirical Findings; Ordnungs Politisches Portal (OPO): Erfurt, Germany, 2020. [Google Scholar]
- Bergqvist, K.; Yngwe, M.; Lundberg, O. Understanding the role of welfare state characteristics for health and inequalities—An analytical review. BMC Public Health 2013, 13, 1234. [Google Scholar] [CrossRef] [PubMed]
- Ferrera, M. The ‘Southern Model’ of Welfare in Social Europe. J. Eur. Soc. Policy 1996, 6, 17–37. [Google Scholar] [CrossRef]
- Minas, C.; Antoniou, E.; McMullan, C.; Jacobson, D. Welfare regime, welfare pillar and southern Europe. J. Eur. Soc. Policy 2014, 24, 135–149. [Google Scholar] [CrossRef]
- Aidukaite, J. Old welfare state theories and new welfare regimes in Eastern Europe: Challenges and implications. Communist Post-Communist Stud. 2009, 42, 23–39. [Google Scholar] [CrossRef]
- Chung, H.; Ng, E.; Ibrahim, S.; Karlsson, B.; Benach, J.; Espelt, A.; Muntaner, C. Welfare State Regimes, Gender, and Depression: A Multilevel Analysis of Middle and High Income Countries. Int. J. Environ. Res. Public Health 2013, 10, 1324–1341. [Google Scholar] [CrossRef]
- Emmenegger, P.; Kvist, J.; Marx, P.; Petersen, K. Three Worlds of Welfare Capitalism: The making of a classic. J. Eur. Soc. Policy 2015, 25, 3–13. [Google Scholar] [CrossRef]
- Kammer, A.; Niehues, J.; Peichl, A. Welfare regimes and welfare state outcomes in Europe. J. Eur. Soc. Policy 2012, 22, 455–471. [Google Scholar] [CrossRef]
- Saint-Arnaud, S.; Bernard, P. Convergence or Resilience? A Hierarchical Cluster Analysis of the Welfare Regimes in Advanced Countries. Curr. Sociol. 2003, 51, 499–527. [Google Scholar] [CrossRef]
- Soede, A.J.; Vrooman, J.C.; Ferraresi, P.M.; Segre, G. Unequal Welfare States; Social Cultural Planning Office: The Hague, The Netherlands, 2004. [Google Scholar]
- Shalev, M. Limits and alternatives to multiple regression in comparative research. In Capitalisms Compared; Emerald Group Publishing Limited: Bingley, UK, 2007; pp. 261–308. [Google Scholar]
- Ferragina, E.; Seeleib-Kaiser, M. Thematic Review: Welfare regime debate: Past, present, futures? Policy Politics 2011, 39, 583–611. [Google Scholar] [CrossRef] [Green Version]
- Ebbinghaus, B. Comparing Welfare State Regimes: Are Typologies an Ideal or Realistic Strategy; ESPAN: Edinburg, UK, 2012; pp. 1–20. [Google Scholar]
- Brennenstuhl, S.; Quesnel-Vallée, A.; McDonough, P. Welfare regimes, population health and health inequalities: A research synthesis. J. Epidemiol. Community Health 2011, 66, 397–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]





| Variables | N | All | Nordic (N = 7722) | Bismarckian (N = 9793) | Anglo-Saxon (N = 4804) | Southern (N = 5944) | Eastern (N = 15,289) |
|---|---|---|---|---|---|---|---|
| Sociodemographics | N | Percentage | |||||
| Gender | |||||||
| Female | 23,374 | 53.7 | 49.2 | 51.7 | 54.7 | 55.7 | 56.1 |
| Age | |||||||
| 18–29 | 6917 | 15.9 | 17.6 | 15.3 | 15.2 | 15.5 | 15.8 |
| 30–39 | 6901 | 15.9 | 15.4 | 14.4 | 17.8 | 17.4 | 15.8 |
| 40–49 | 7679 | 17.6 | 17.2 | 18.9 | 17.5 | 17.3 | 17.2 |
| 50–59 | 7804 | 17.9 | 17.9 | 18.5 | 16.1 | 16.9 | 18.5 |
| 60–69 | 7263 | 16.7 | 17.3 | 16.3 | 16.4 | 15.7 | 17.1 |
| 70–79 | 4930 | 11.3 | 10.3 | 11.2 | 11.2 | 11.8 | 11.7 |
| 80+ | 2058 | 4.7 | 4.3 | 5.4 | 5.9 | 5.4 | 3.9 |
| MWB | N | Mean (standard deviation) | |||||
| SWB | 42,377 | 3.6 (0.7) | 3.9 (0.6) | 3.8 (0.6) | 3.5 (0.8) | 3.4 (0.8) | 3.6 (0.7) |
| PWB | 41,152 | 4.0 (0.5) | 4.1 (0.4) | 4.1 (0.4) | 4.0 (0.5) | 4.0 (0.5) | 3.9 (0.5) |
| Model 0 | Model 1 WS Index | Model 2 WS Factors | Model 3 WS Regimes | |||||
|---|---|---|---|---|---|---|---|---|
| SWB | PWB | SWB | PWB | SWB | PWB | SWB | PWB | |
| Gender (ref Male) | ||||||||
| Female | −0.066 *** | −0.013 | −0.06 *** | −0.011 | −0.06 *** | −0.011 | −0.06 *** | −0.01 |
| Age-groups (ref 18–29) | Ref: Nordic | |||||||
| 30–39 | −0.072 *** | −0.0062 | −0.076 *** | −0.0082 | −0.076 *** | −0.0076 | −0.043 | −0.0015 |
| 40–49 | −0.16 *** | −0.030 * | −0.16 *** | −0.032 ** | −0.16 *** | −0.031 ** | −0.042 ** | 0.019 |
| 50–59 | −0.21 *** | −0.028 | −0.22 *** | −0.032 * | −0.22 *** | −0.032 * | −0.012 | 0.0096 |
| 60–69 | −0.17 *** | −0.0099 | −0.19 *** | −0.02 | −0.19 *** | −0.019 | 0.073 | 0.043 ** |
| 70–79 | −0.20 *** | −0.045 | −0.22 *** | −0.057 * | −0.22 *** | −0.057 * | 0.058 | 0.034 |
| 80+ | −0.26 *** | −0.10 * | −0.29 *** | −0.12 *** | −0.30 *** | −0.13 *** | −0.033 | −0.073 |
| Welfare state and age-interactions | ||||||||
| X1 = WS index | X1 = WS factor 1 | X1 = Bismarckian | ||||||
| X1 | 0.099 *** | 0.017 | 0.054 * | 0.02 | −0.053 | −0.022 | ||
| X1•30–39 | 0.0082 | 0.0062 | 0.0067 | 0.0071 | −0.011 | 0.00037 | ||
| X1•40–49 | 0.074 *** | 0.031 ** | 0.063 *** | 0.027 * | −0.04 | −0.021 | ||
| X1•50–59 | 0.15 *** | 0.048 *** | 0.11 *** | 0.038 ** | −0.11 * | −0.0033 | ||
| X1•60–69 | 0.22 *** | 0.097 *** | 0.18 *** | 0.099 *** | −0.094 | 0.035 | ||
| X1•70–79 | 0.24 *** | 0.12 *** | 0.20 *** | 0.12 *** | −0.092 | 0.025 | ||
| X1•80+ | 0.22 *** | 0.13 *** | 0.18 *** | 0.15 *** | −0.15 ** | 0.069 | ||
| X2 = WS factor 2 | X2 = Anglo-Saxon | |||||||
| X2 | 0.087 *** | 0.00094 | −0.18 *** | −0.13 *** | ||||
| X2•30–39 | 0.0051 | 0.0028 | −0.047 | 0.018 | ||||
| X2•40–49 | 0.042 * | 0.018 | −0.16 *** | −0.062 ** | ||||
| X2•50–59 | 0.11 *** | 0.030* | −0.072 | 0.054 | ||||
| X2•60–69 | 0.14 *** | 0.037 | −0.014 | 0.13 *** | ||||
| X2•70–79 | 0.15 *** | 0.053 | −0.02 | 0.12 *** | ||||
| X2•80+ | 0.14 *** | 0.044 | 0.11 ** | 0.25 *** | ||||
| X3 = Southern | ||||||||
| X3 | −0.20 *** | −0.0097 | ||||||
| X3•30–39 | −0.081 * | −0.015 | ||||||
| X3•40–49 | −0.16 *** | −0.052 | ||||||
| X3•50–59 | −0.28 *** | −0.066 | ||||||
| X3•60–69 | −0.35 *** | −0.065 | ||||||
| X3•70–79 | −0.33 ** | −0.095 | ||||||
| X3•80+ | −0.32 * | −0.045 | ||||||
| X4 = Eastern | ||||||||
| X4 | −0.19 ** | −0.064 | ||||||
| X4•30–39 | −0.035 | −0.017 | ||||||
| X4•40–49 | −0.18 *** | −0.083 ** | ||||||
| X4•50–59 | −0.36 *** | −0.098 *** | ||||||
| X4•60–69 | −0.51 *** | −0.19 *** | ||||||
| X4•70–79 | −0.55 *** | −0.24 *** | ||||||
| X4•80+ | −0.50 *** | −0.23 *** | ||||||
| Constant | 3.82 *** | 4.06 *** | 3.80 *** | 4.05 *** | 3.80 *** | 4.05 *** | 3.94 *** | 4.10 *** |
| ICC (se) | 0.101 (0.022) | 0.045 (0.013) | 0.031 (0.007) | 0.03 (0.007) | 0.028 (0.008) | 0.029 (0.007) | 0.042 (0.01) | 0.027 (0.006) |
| R2 country-level (SB/BR) | 0.72/0.72 | 0.33/0.34 | 0.75/0.75 | 0.37/0.38 | 0.62/0.62 | 0.41/0.41 | ||
| AIC | 87,278.25 | 53,137.62 | 86,575.33 | 52,818.1 | 86,566.72 | 52,757.2 | 86,554.9 | 52,691.87 |
| BIC | 87,364.8 | 53,223.87 | 86,722.46 | 52,964.73 | 86,774.42 | 52,964.2 | 86,883.76 | 53,019.62 |
| N | 42,377 | 41,152 | 42,377 | 41,152 | 42,377 | 41,152 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalseth, J.; Donisi, V.; Miret, M.; Forsman, A.K.; Cresswell-Smith, J. Exploring the Association between Welfare State and Mental Wellbeing in Europe: Does Age Matter? Int. J. Environ. Res. Public Health 2022, 19, 10985. https://doi.org/10.3390/ijerph191710985
Kalseth J, Donisi V, Miret M, Forsman AK, Cresswell-Smith J. Exploring the Association between Welfare State and Mental Wellbeing in Europe: Does Age Matter? International Journal of Environmental Research and Public Health. 2022; 19(17):10985. https://doi.org/10.3390/ijerph191710985
Chicago/Turabian StyleKalseth, Jorid, Valeria Donisi, Marta Miret, Anna K. Forsman, and Johanna Cresswell-Smith. 2022. "Exploring the Association between Welfare State and Mental Wellbeing in Europe: Does Age Matter?" International Journal of Environmental Research and Public Health 19, no. 17: 10985. https://doi.org/10.3390/ijerph191710985