1. Introduction
The oldest old population, defined here as adults aged 80 years and over [
1] is projected to rise globally from 143 million in 2019 to 426 million by 2050 [
2]. This demographic transition has stimulated broad discussions regarding the need for age-friendly environments [
3]. Mental wellbeing is an important area of focus in this regard, with links to positive health outcomes [
4], increased life expectancy [
5] and economic benefits [
6,
7,
8]. Our daily environments are shaped by the surrounding welfare state policies, which in turn, impact mental wellbeing also in oldest old age [
9].
Definitions of mental wellbeing differ according to which distinct features and dimensions are emphasised [
10]. Subjective wellbeing [
11] approaches tend to emphasise the evaluative dimension of wellbeing with a focus on cognitive appraisals of life satisfaction, together with the hedonic or emotional dimension, which relates to a sense of pleasure and happiness [
12,
13,
14]. Eudaimonic approaches, on the other hand, emphasise the importance of meaning, for example, via personal development and self-realisation. These approaches include Ryff’s definition of psychological wellbeing made up of life purpose, mastery and positive relatedness, flow, autonomy, personal growth and self-acceptance [
15].
Keyes’ model [
16,
17] is built in relation to factors that influence flourishing and languishing, while Seligman’s PERMA model builds on five components, including positive emotions, engagement, relationships, meaning and accomplishment [
18]. Approaching mental wellbeing as a multidimensional construct allows for a comprehensive understanding [
19,
20].
Exploring different dimensions of mental wellbeing sheds light on phenomenon, such as the ‘wellbeing paradox’, denoting a tendency for the evaluative dimension to increase in older age, particularly in the context of wealthier, English speaking countries [
21]. Socio-economic or socio-political context appears to lie behind this paradox, as the effect has not been replicated in lower income countries or in post-communist countries [
22]. Different aspects of wellbeing tend to vary according to age group and what dimensions of wellbeing are under consideration as well as on the individual characteristics and life circumstances of the study participants [
23]. Furthermore, specific aspects of a country’s social policy have been found to influence wellbeing [
23].
For example, high levels of emotional wellbeing (happiness) have been attributed to the influence of welfare state in Nordic countries [
24] as have high levels of flourishing [
25]. Wellbeing may be influenced by characteristics, such as low income inequality, high social trust and well-developed social welfare and health care systems [
26]. These approaches parallel research on the importance of social determinants of mental health [
27]. In line with this, the Mental Wellbeing Impact Assessment (MWIA) framework proposes four protective pathways for mental wellbeing—namely enhancing control, increasing resilience and community assets, facilitating participation and promoting inclusion [
28].
Despite constituting a growing segment of the population, the oldest old age group tends to be overlooked in research [
29,
30]. In a step towards ameliorating this research gap, the European Welfare Models and Mental Wellbeing in Final Years of Life (EMMY) project (
www.emmyproject.eu) used a mixed-methods approach to explore mental wellbeing in the oldest old age group. The EMMY project (2017–2019) made use of data from Round 6 of the European Social Survey (ESS). These included data from rotating modules on personal and social wellbeing and a broad range of items related to MWB [
31].
Exploratory factor analysis [
32] highlighted five important dimensions of mental wellbeing in oldest old age (1) the evaluative dimension capturing overall happiness and life-satisfaction; (2) the emotional dimension including enjoyment, calmness and happiness; (3) positive psychological functioning, built on autonomy, competence, self-esteem and optimism; (4) meaning and flow, describing states of presence and engagement; and (5) positive and supportive relationships that is, giving and receiving support and feeling appreciated [
33]. A further paper originating from the EMMY project found that a welfare state mattered more for mental wellbeing in older age groups compared to younger age groups [
9].
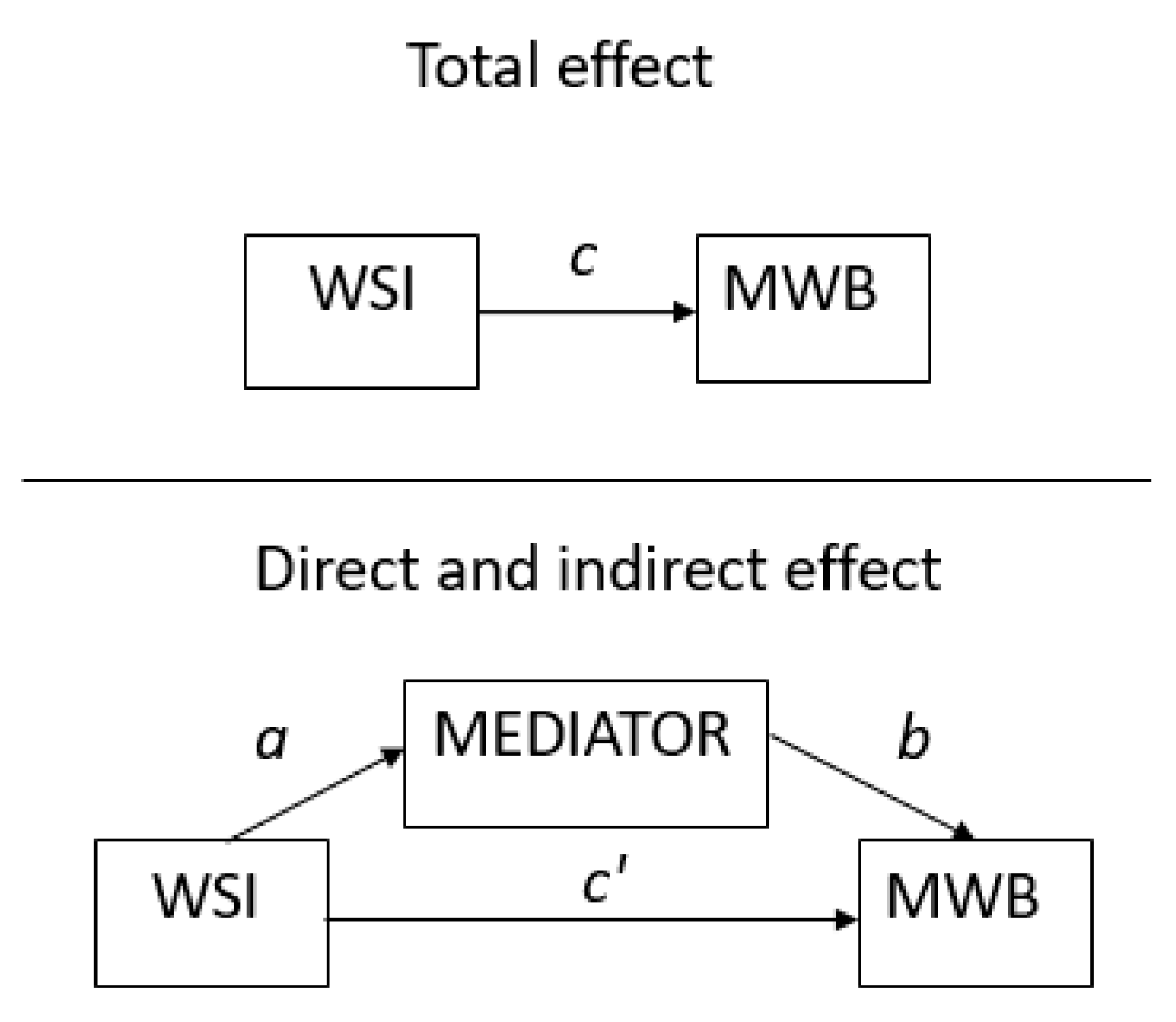
The current paper explores how the conditions of daily life influence the different dimensions of mental wellbeing in the oldest old age. More specifically we look at the mediating effect of these variables on the welfare state effect in terms of five dimensions of mental wellbeing. Teasing out the influence of these variables gives us a better understanding of the drivers of mental wellbeing in oldest old age, facilitating evidence to inform policy making for this growing population group.
4. Discussion
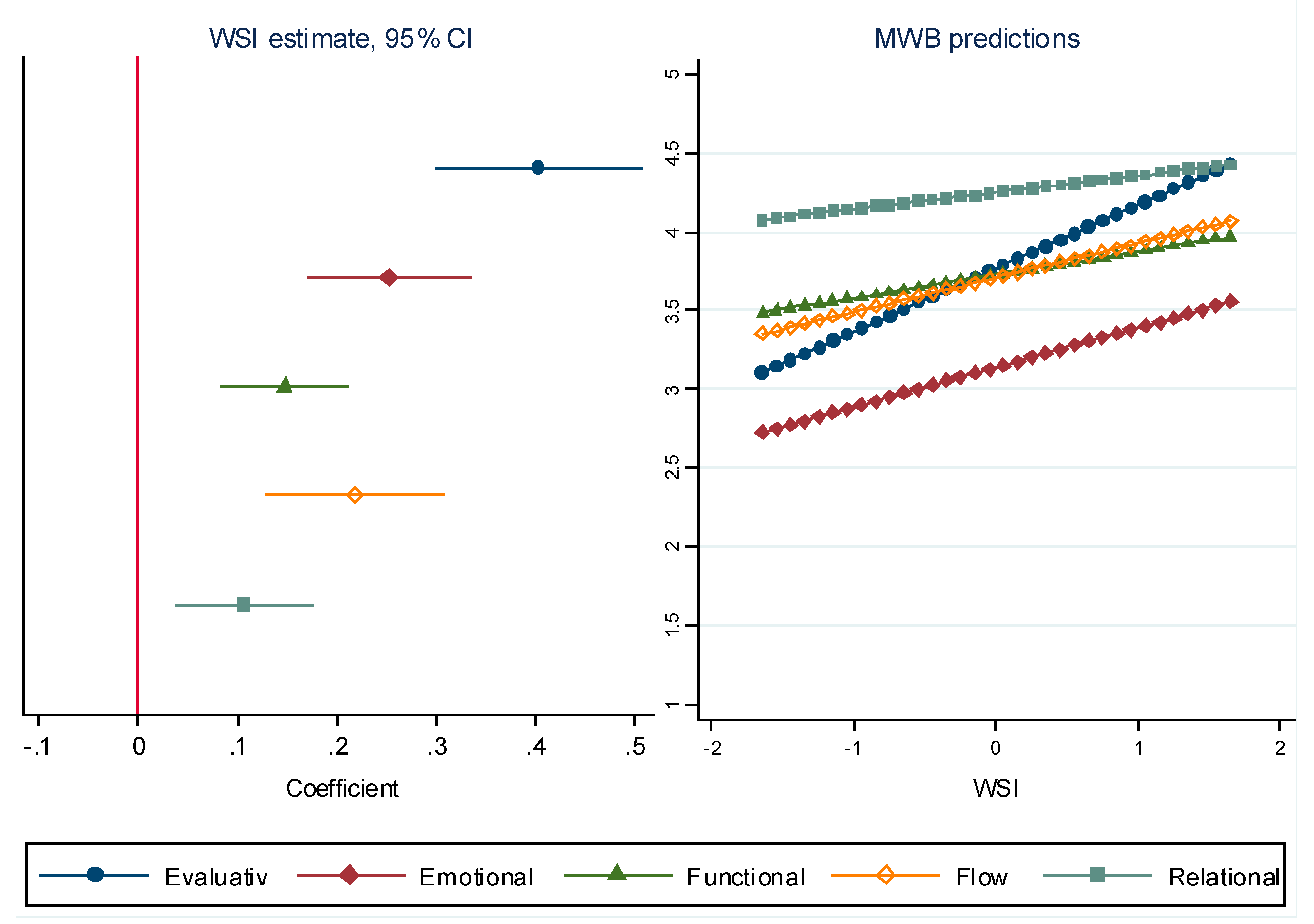
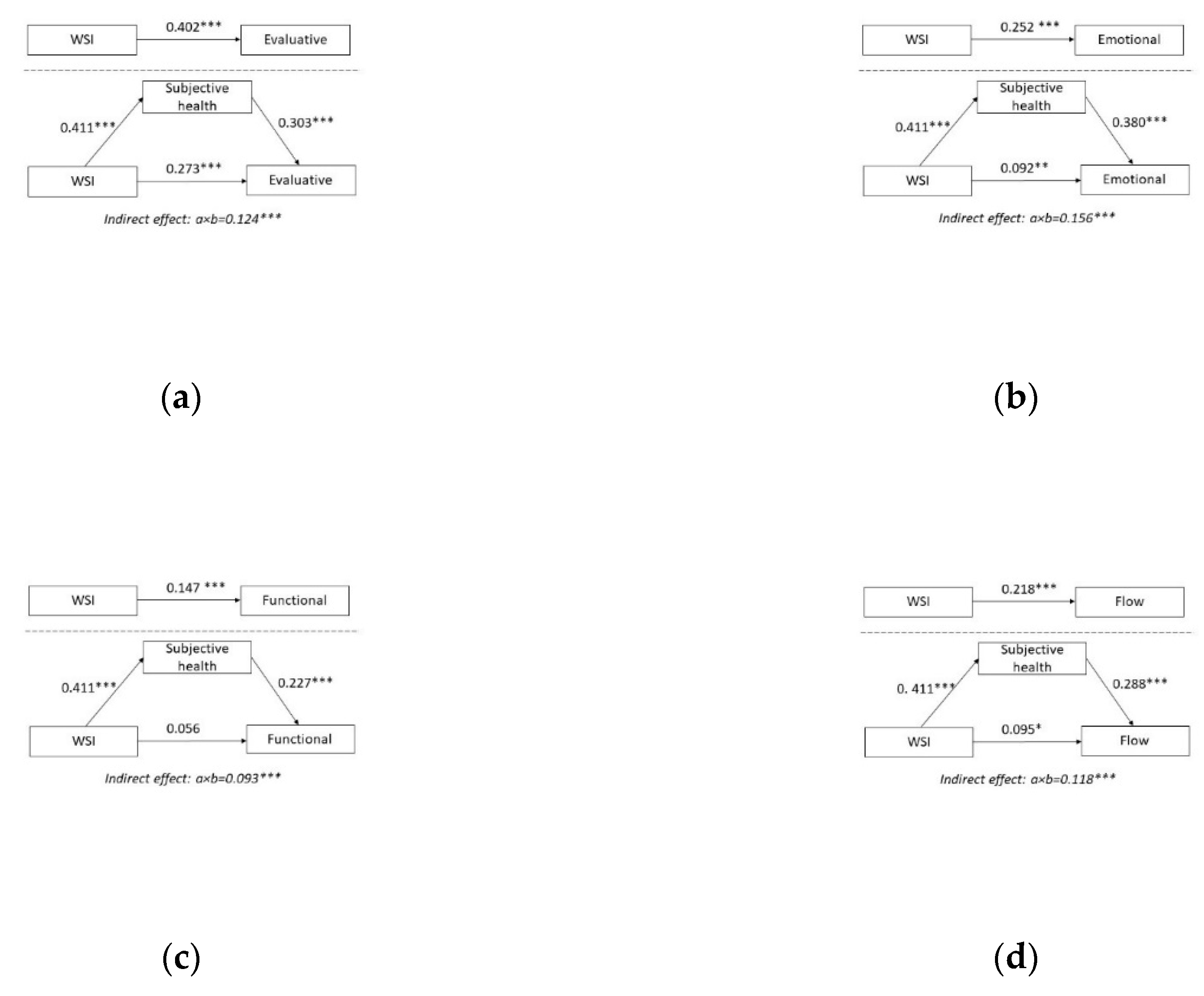
The results identify important mediators of the welfare state effect on five different dimensions of mental wellbeing in oldest old age. Our study confirms that higher levels of the WSI are associated with higher the levels of different dimensions of mental wellbeing. Furthermore, by exploring how the conditions of daily life mediate the welfare state effect in relation to these dimensions, three areas were found to be particularly influential: subjective general health, coping with income and place in society each impacted specific dimensions of mental wellbeing differently.
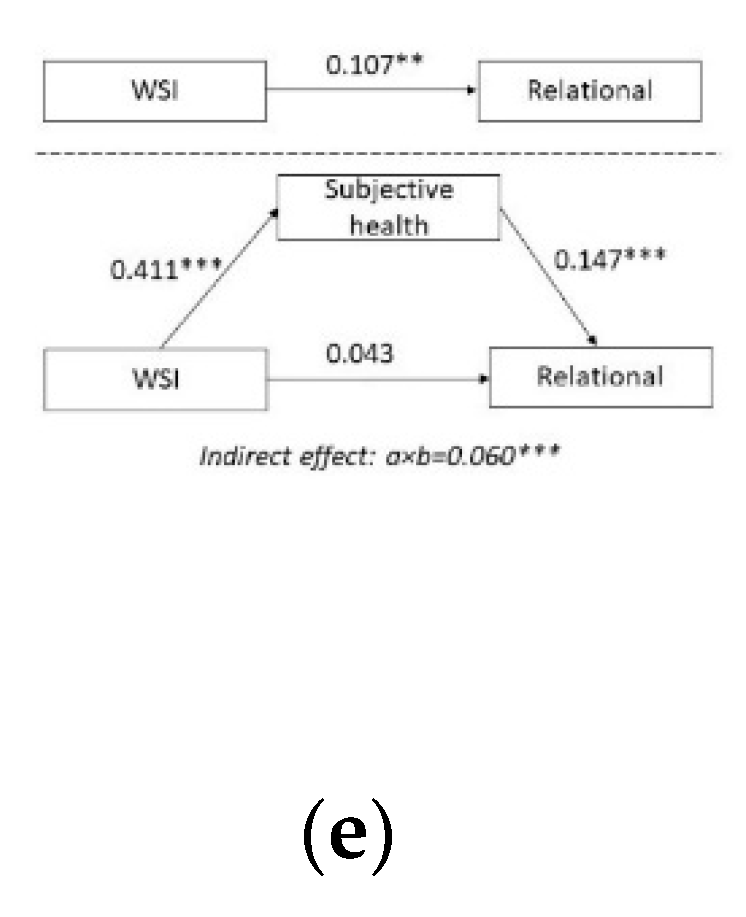
4.1. Subjective General Health and Mental Wellbeing
Health is especially important in oldest old age due to the higher likelihood of illness and increased support needs [
41]. Older adults are often reliant on support, such as care and pension provisions for their wellbeing, which simultaneously serve to ameliorate health inequalities [
42]. The current study found higher levels of subjective general health in stronger welfare states compared with less developed welfare states. The welfare state effect can therefore be considered to be significantly influenced by levels of subjective general health.
Previous studies highlight the need for promoting health in order to improve life satisfaction, especially in economically disadvantaged population groups [
43]. There is a positive correlation between subjective health and the emotional dimension of wellbeing. Declining health status in old age does not always produce a similar decline in the emotional dimension of mental wellbeing [
21]. Despite the majority of people reaching oldest old age with multiple health difficulties, they still tend to report high levels of self-reported health, which may potentially be a reflection of psychological adaptation [
44].
It remains unclear whether the association between this positive subjective assessment and the strength of the welfare state is due to stronger psychological adaptation, fewer health-related concerns due to better access to public services or some other contextual factor linked to the welfare state. Although the exact mechanisms are objects for further studies, the end result remains the same, which is higher levels of mental wellbeing among the oldest old in stronger welfare states.
Similarly, the considerable influence of subjective health in relation to the psychological functioning dimension of mental wellbeing was demonstrated by the welfare state effect diminishing significantly (achieving full mediation) when subjective health was added to the mediation model. Positive subjective health appears to therefore support the psychological functioning dimension of mental wellbeing in oldest old age. Items making up the psychological functioning dimension have links to aspects of autonomy. Previous research also emphasised the importance of autonomy in older age, although highlighting that support may be necessary in accordance with age-related needs [
45].
Therefore, welfare states that support health in oldest old age may simultaneously support a sense of autonomy. The flow dimension of mental wellbeing was also mediated by the subjective health variable and was higher in countries with stronger welfare state support. Supporting subjective health appears to therefore strengthen a feeling of meaning and engagement in oldest old age. Importantly, previous research underlined the ability derive enjoyment from daily activities despite health difficulties [
46].
Subjective general health almost fully mediated the welfare state effect on the relational dimension. A good level of health was also found to be a protective factor against loneliness for people aged 60 years and over in a previous study [
47]. Relationships are particularly important in oldest old age considering the higher risk of isolation and loneliness, for example, via the age-related losses of partners, siblings or friends [
48].
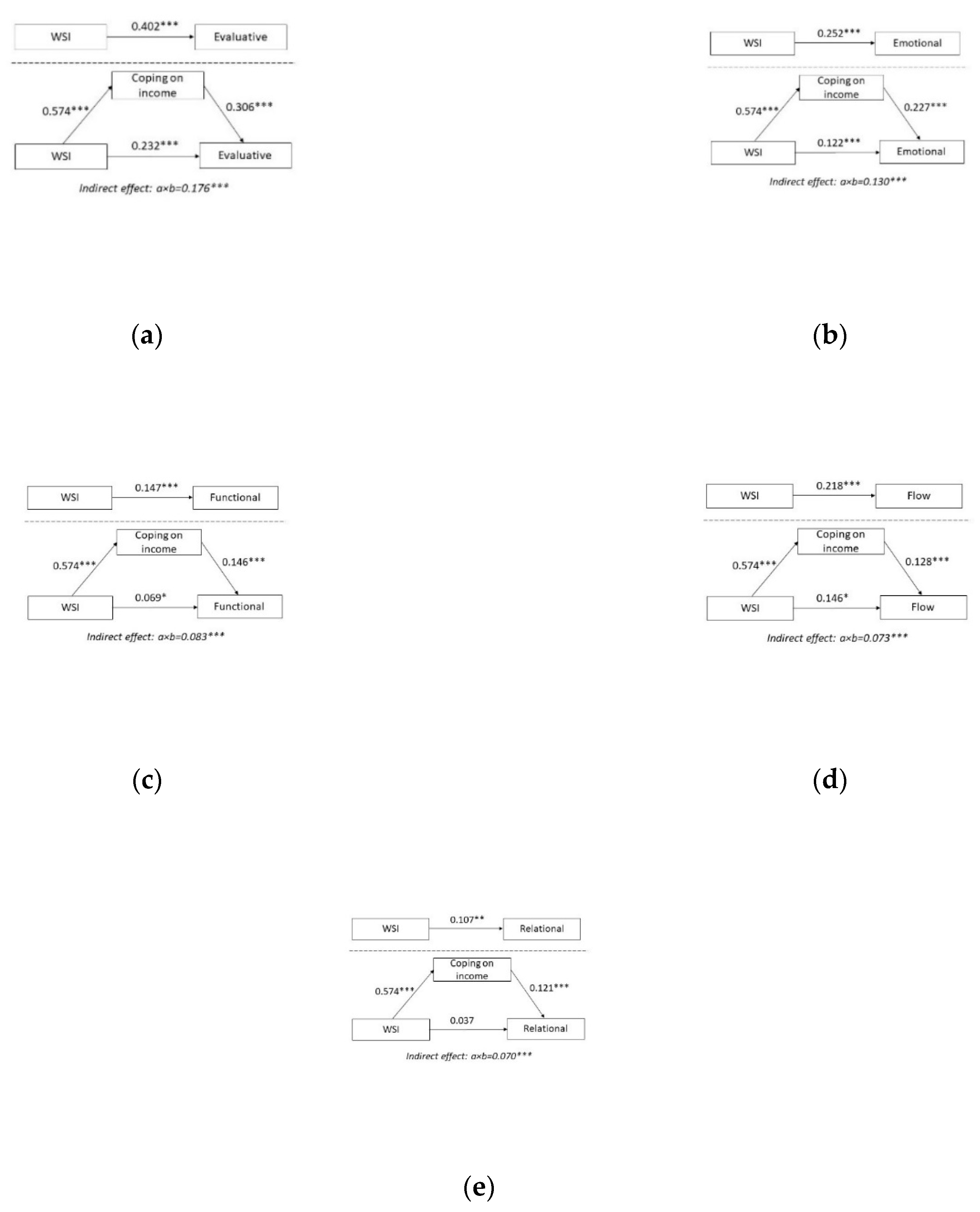
4.2. Coping with Income and Mental Wellbeing
The basic purpose of the welfare state is to provide economic security and social equality, for example via social transfers, such as pensions. The current study found the welfare state effect on all dimensions of mental wellbeing to be mediated by the coping with income variable. Interestingly, the coping with income variable increased most with each incremental increase in WSI. Although research suggests that older adults report comparatively less financial difficulty than younger age groups, welfare state support appears to be especially important for individuals with higher support needs [
49]. Income redistribution is one important aspect of welfare states; however, an equally important aspect of welfare states is access to non-income benefits and services.
The coping with income variable had the strongest impact on the evaluative and emotional dimension of mental wellbeing. Although using different measures of income and a younger age group, previous research indicated that income tends to influence the evaluative and the emotional dimensions differently [
50]. Although specific reasons behind these differences lie outside of the scope of this article, it does appear that the welfare state effect is mediated by income for both dimensions also in the oldest old age group. Coping with one’s current income mediates the welfare state effect on the psychological functioning dimension, implying that that having a subjective sense of financial security impacts autonomy and a sense of accomplishment in oldest old age. A welfare state can support autonomy by ensuing that older adults have sufficient income to access what they need for a good life.
A preference for ‘ageing in place’—that is, remaining living in the home environment as long as possible [
51], has been found to foster independence and allow for higher levels of control and a higher quality of life [
52]. A welfare state can facilitate ageing in place by ensuring adequate income, suitable housing options, access to services and social support within and outside of the home [
53]. It is equally important to ensure autonomy within the context of residential care in terms of people’s decisions about their daily activities, maintaining dignity and upholding human rights [
54,
55]. Welfare state support is especially important in relation to high support needs. Financial deterrents are more likely in countries where individuals are expected to make their own contributions to institutional care, which tend to only take place only when it is absolutely necessary [
56].
The mediation effect on the flow dimension illustrates how a subjective sense of financial security influences feelings of being interested, absorbed and enthusiastic. Longitudinal benefits of economic wellbeing in younger age groups indicates that higher income and/or increases in income are associated with higher levels of certain aspects of psychological wellbeing, such as purpose in life, self-acceptance, personal grown and environmental mastery, paralleling findings from the current study [
57]. Ensuring access to leisure activities in oldest old age may be done by ensuring adequate transport and mobility [
58] and access to day centres [
59] or leisure activities [
60].
The coping with income variable almost fully mediated the welfare state effect on the relational dimension suggesting that a subjective sense of financial security promotes a sense of being treated with respect, of being appreciated as well as providing and receiving help and support. The relational dimension was least affected by differing levels of welfare state support (see
Figure 3). The link between having an adequate income and the relational dimension seems logical in the oldest old age considering that oldest old age is a time when support needs are likely to increase [
9]. With less support from the welfare state, family relations and family financial support become critical, especially in the context of inadequate income levels. Intergenerational family support is more likely to be unbalanced and non-reciprocal in low-income contexts. Circumstances in which the older adult is predominantly the recipient of support from family members has been linked to lower levels of life satisfaction [
61].
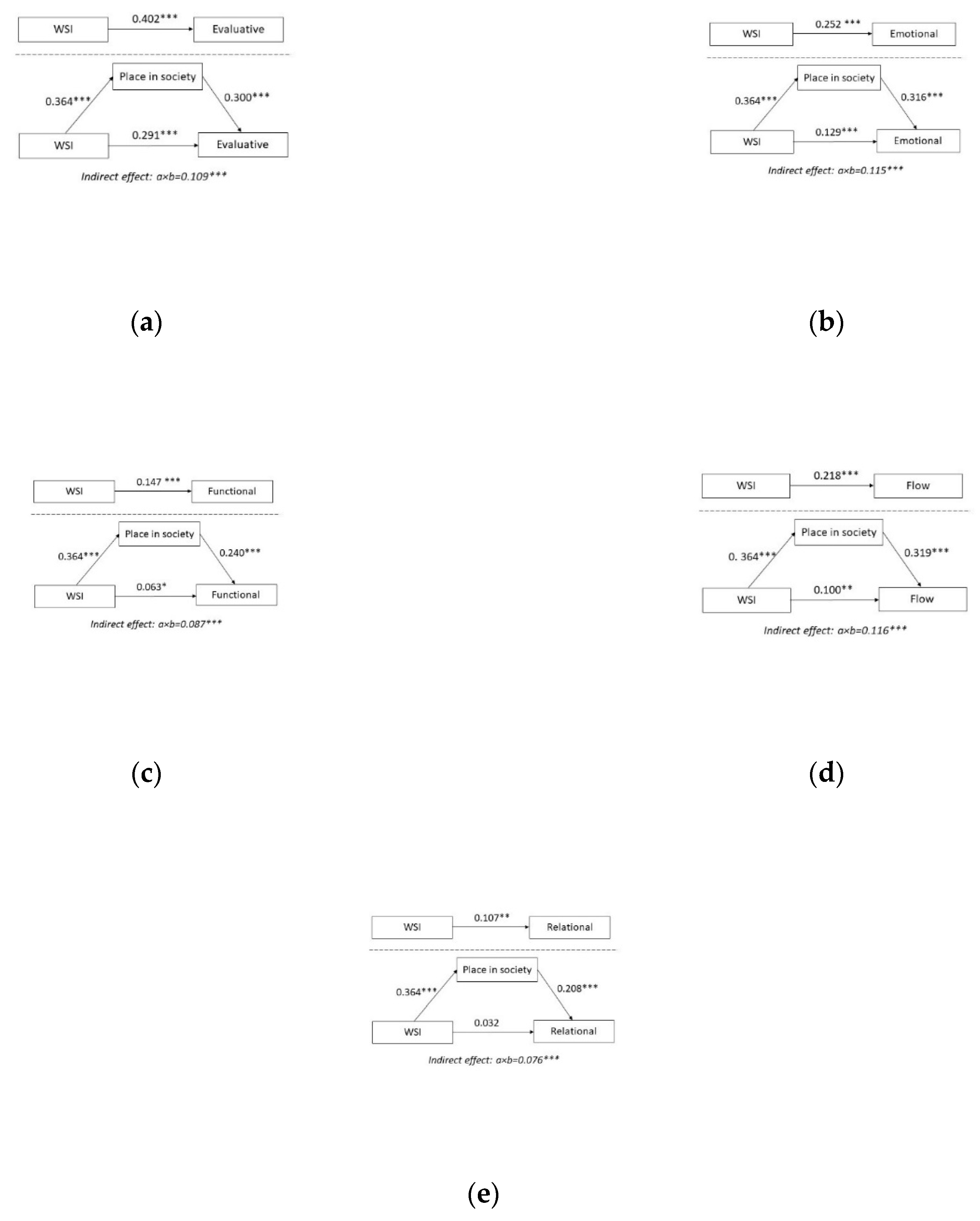
4.3. Place in Society and Mental Wellbeing
The positive association between status and subjective well-being in the general population is well-documented in previous research [
62]. Subjective social status—that is, how people perceive their place in society—has been reported to have links to health and mental health outcomes [
63] also in old age [
64]. These associations have been found to persist even when statistically accounting for socioeconomic indicators, such as income, education and occupational prestige confirming the usefulness of the subjective measure [
65]. Furthermore, cross country comparisons suggest that the health benefits related to high levels of subjective social status appears to be slightly more prominent in more affluent countries [
65].
Welfare generosity (represented here by higher WSI values) aims to decrease poverty and increase equity by redistributing resources through social welfare and social protection. The current study showed a strong welfare state effect for the place in society variable, indicating that participants from countries with a higher WSI also reported a higher level of perceived placement in society. The place in society variable had a significant indirect effect on all mental wellbeing dimensions, implying a broad influence on the welfare state effect in this regard. A positive correlation between status and subjective wellbeing was previously reported in an age group under the age of 80 [
66]. High levels of subjective social-economic status have also been reported in relation to mental wellbeing in older age groups, although less attention has been given to individual dimensions [
67,
68].
The current study found the place in society variable to explain part of the welfare state in terms of the evaluative dimension. Similarly, actions aiming to improve social status (for example by reducing social inequality) have been found to improve life satisfaction in the general population [
69]. The current study also found place in society to influence the emotional dimension. Our findings parallel previous studies reporting the subjective position in society to be an important predictor of happiness in the general age group [
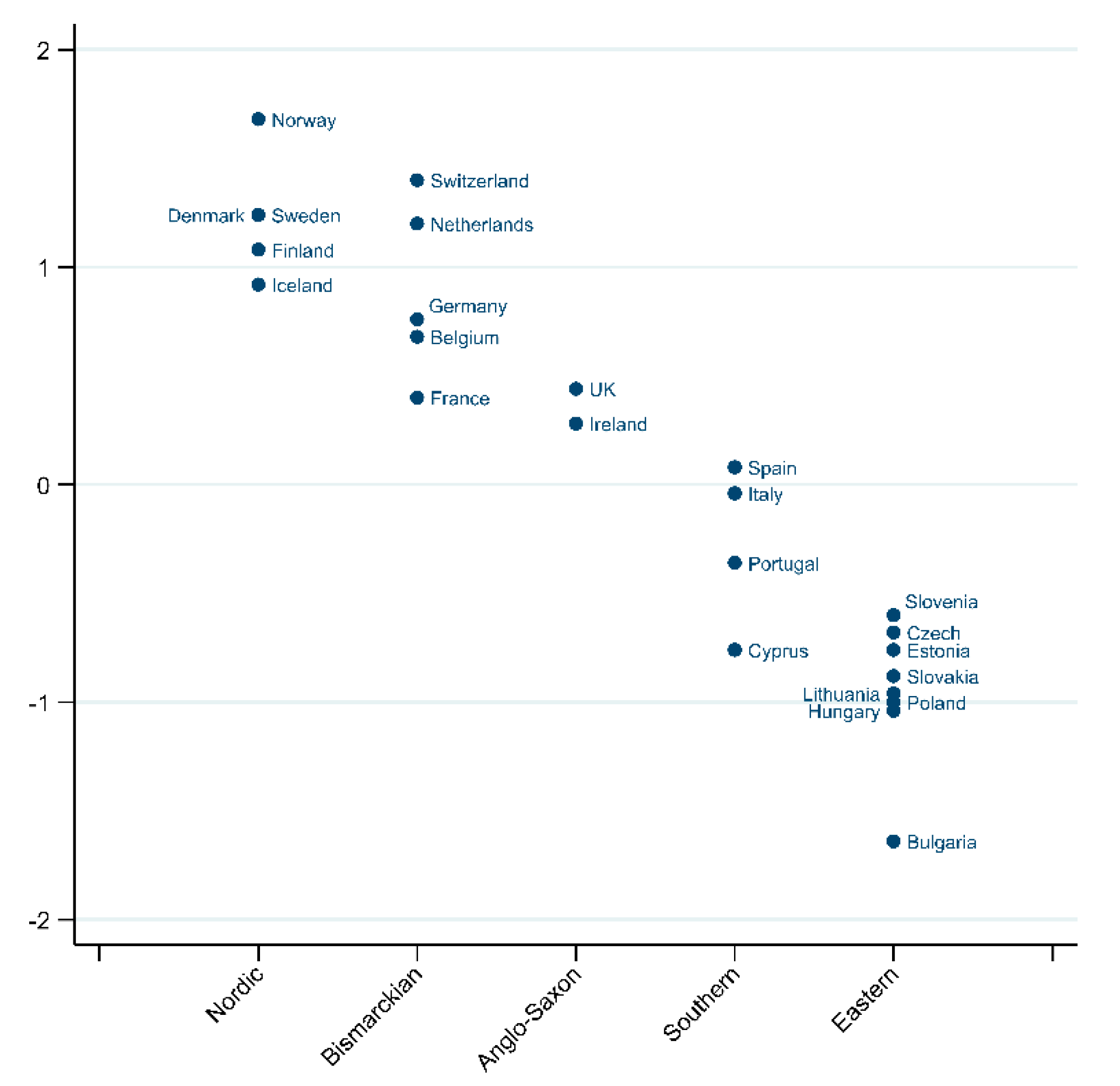
24]. This was also found to be moderated by the welfare state, although to a lesser extent in the context of the Nordic countries compared to Eastern European countries [
24].
The place in society variable also mediated the welfare state effect on the psychological functioning dimension in the current study. More equitable welfare states with higher levels of resources can be assumed to support the psychological functioning dimension of mental wellbeing. This is of particular relevance in older age as this age group tends to be ascribed low social status, and ageist attitudes are pervasive in many countries [
70]. Ageism and associated negative health outcomes have been found to be more prevalent in countries with lower level of resources [
71] and a high percentage of older adults [
72].
The place in society item also mediated the welfare state effect on the flow dimension, which could potentially be stimulated by a variety of community activities, including voluntary or charity work, educational or training courses, sport, social or other kind of clubs and political or community-related organisations. All of these have been shown to follow a social gradient, with a higher social position increasing the likelihood of engagement in community activities among older people [
73]. Studies also indicate that facilitating these actions impacts how engaged older adults are in these activities [
74]. Furthermore, the place of society variable fully mediated the welfare state effect the relational dimension, highlighting an association between subjective social status and a sense of being treated with respect, feeling appreciated and being able to provide help and support.
The current study implies that life conditions in the daily environment has a mediating effect on many dimensions of mental wellbeing in oldest old age. Although three main variables were picked out in more detail, other variables also paint a similar picture. The variable ‘learn new things’ mediated the welfare state effect on all dimensions of mental wellbeing. Life-long learning is an area of limited attention in the oldest old age group. The results from this study could potentially provide a springboard for further study.
4.4. Protective Factors for Mental Wellbeing in Oldest Old Age; Some Policy Considerations
Building age-friendly environments may require increased attention to the smaller details in life. The World Health Organisation (WHO) highlights the need for facilitating access to activities, such as outdoor environments, social participation including community exchange and lifelong learning, social and neighbourhood cohesion and civic engagement also in old age [
75]. By pinpointing the importance of different life conditions for mental wellbeing, the current study gains insight and support for policy actions, which develop mentally healthy environments for the oldest old. The results also highlight the need for a Mental Health in all Policies (MHiAP) [
76] approach and the importance of involving multiple sectors, such as health, long-term care, transport, housing, labour and social services and actions on different levels, such as governmental and statutory services, civil society as well as individuals, communities and families [
77,
78].
The results from the current study also emphasise the multidimensional nature of mental wellbeing and emphasize the welfare state influence on different dimensions. Facilitating the opportunity to engage in actions that support mental wellbeing in all ages and circumstances needs to be driven by supportive policies. Interestingly, all three of the intervening variables discussed here centre around the notion of autonomy. Autonomy is an area highlighted in the MWIA, including enhancing control, facilitating participation and promoting inclusion (see
Table A2). Support autonomy in oldest old age is an important endeavour for welfare states, considering that this age group is at increased risk of being excluded from both services and social contacts [
79].
4.5. Strengths and Limitations
A strength of the study is its focus on an often neglected age group, which is an especially important area of attention considering the ongoing demographic transition. The current study accounts for the complex nature of both welfare state and mental wellbeing by a multidimensional approach using a composite measure of welfare state (WSI) and including five dimensions of mental wellbeing.
There are however some limitations to be taken into consideration. First, the cross-sectional nature of the ESS data increases the risk of cohort effects. ESS-data were collected from the community (as opposed to supported living environments) meaning there is a bias towards data from people with higher levels of mental wellbeing. Depending on the welfare state structure, individuals with higher health needs are generally more likely to live in institutional care, and it is important to recognise that these individuals are not included in the current data set. Subsequent analyses using longitudinal data could provide further information on cohort and age effects in relation to mental wellbeing and welfare state effects.
Furthermore, the data used in this study are relatively old, stemming from 2012, as this is the last point when the ESS module relating to Subjective and Social Wellbeing was included. It is worth acknowledging that both WS measures and their association to mental wellbeing at different ages may have changed since then. The stability of our results should be tested in later research also looking at longitudinal effects. It would also be useful to repeat these analyses should the ESS repeat the rotating modules used in this study.
It is important to recognise that various perspectives exist in terms of mediation analysis and that statistical models used to test mediation are simply predictive or descriptive and cannot be considered to be inherently causal [
80]. In the case of the current study, we can only conclude that the intervening variables may have an influence in terms of the welfare state effect, but we cannot imply causality. Multiple mediators can be assumed to lie behind the welfare state effect.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}






