
Anorexia Nervosa Is Associated with a Shift to Pro-Atherogenic Low-Density Lipoprotein Subclasses

 ,
,  , , ,
, , ,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment and Group Characteristics
2.1.1. Anthropometry and Body Fat Measurement
2.1.2. Clinical Laboratory Parameters and Adipokines
2.2. Lipoprotein Subclass Analyses with Lipoprint System
2.3. HDL-Associated Proteins and Lipids
2.4. ApoB-Depleted Serum
2.5. Anti-Oxidative Capacity of ApoB-Depleted Serum
2.6. Arylesterase Activity of Paraoxonase 1 (PON1)
2.7. Cholesterol Efflux Capacity of ApoB-Depleted Serum
2.8. LCAT Activity
2.9. CETP Activity
2.10. Statistical Analyses
3. Results
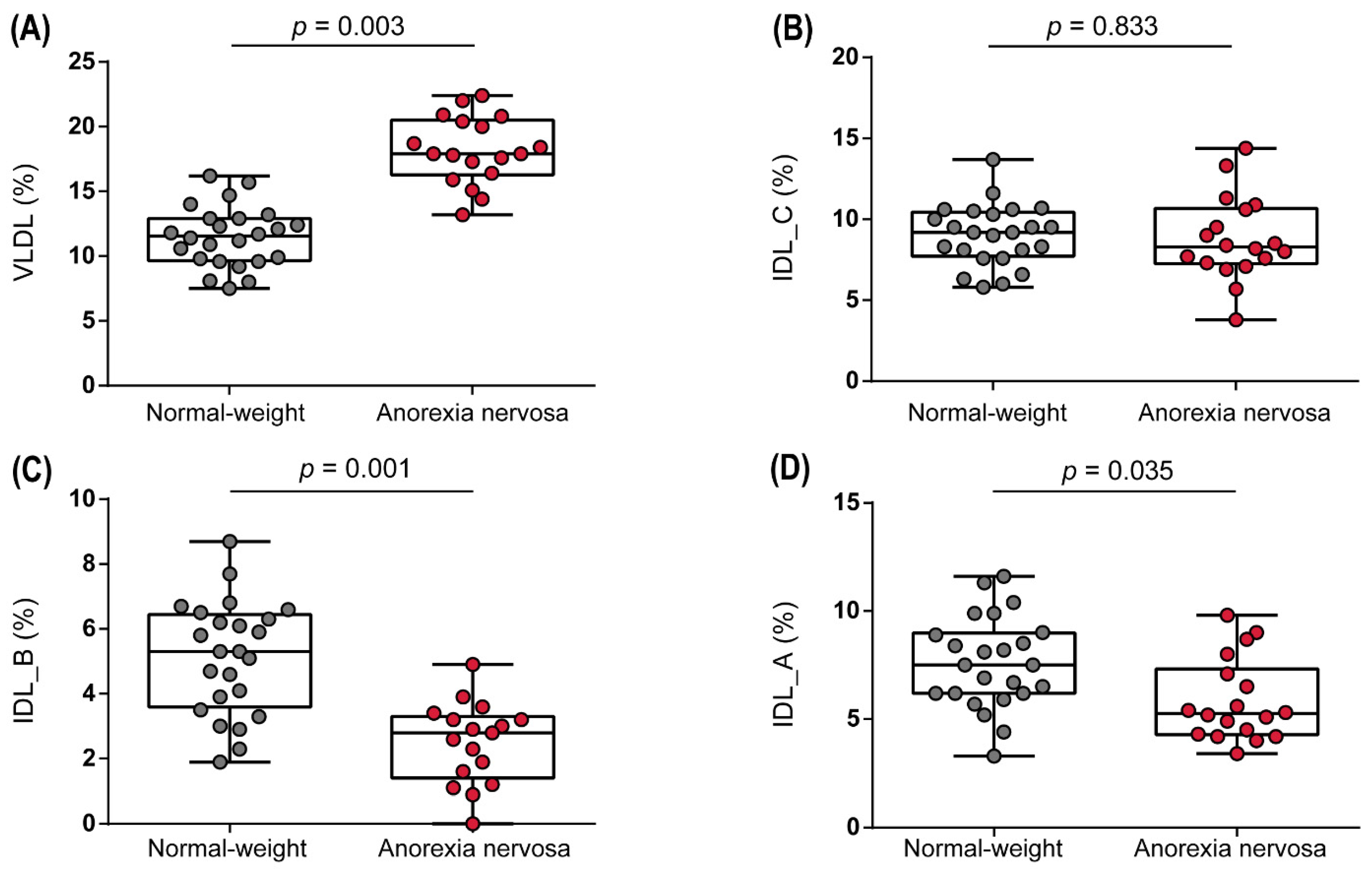
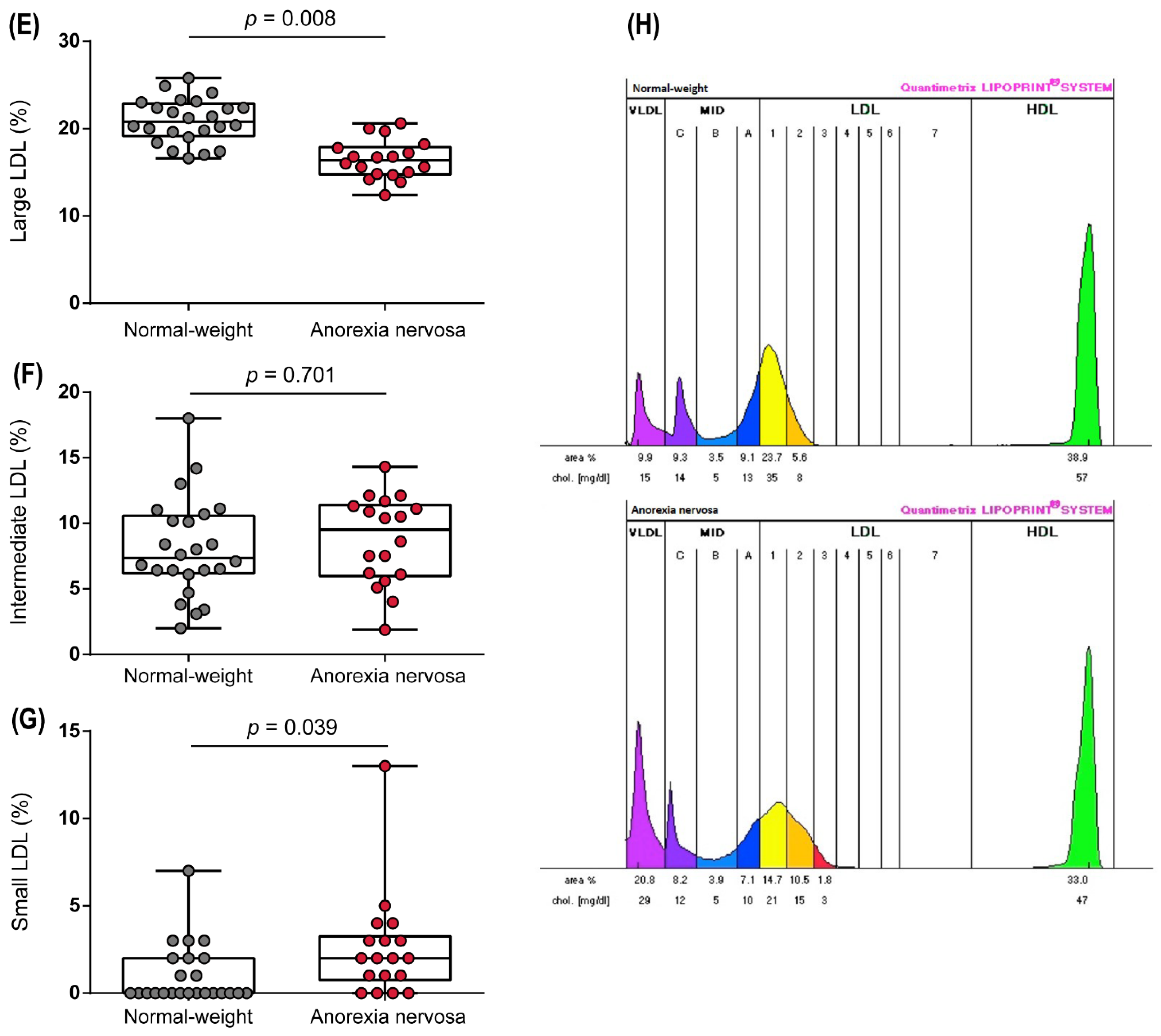
3.1. Anorexia Nervosa Is Associated with Changes in Subclass Distribution of Triglyceride-Rich Lipoproteins
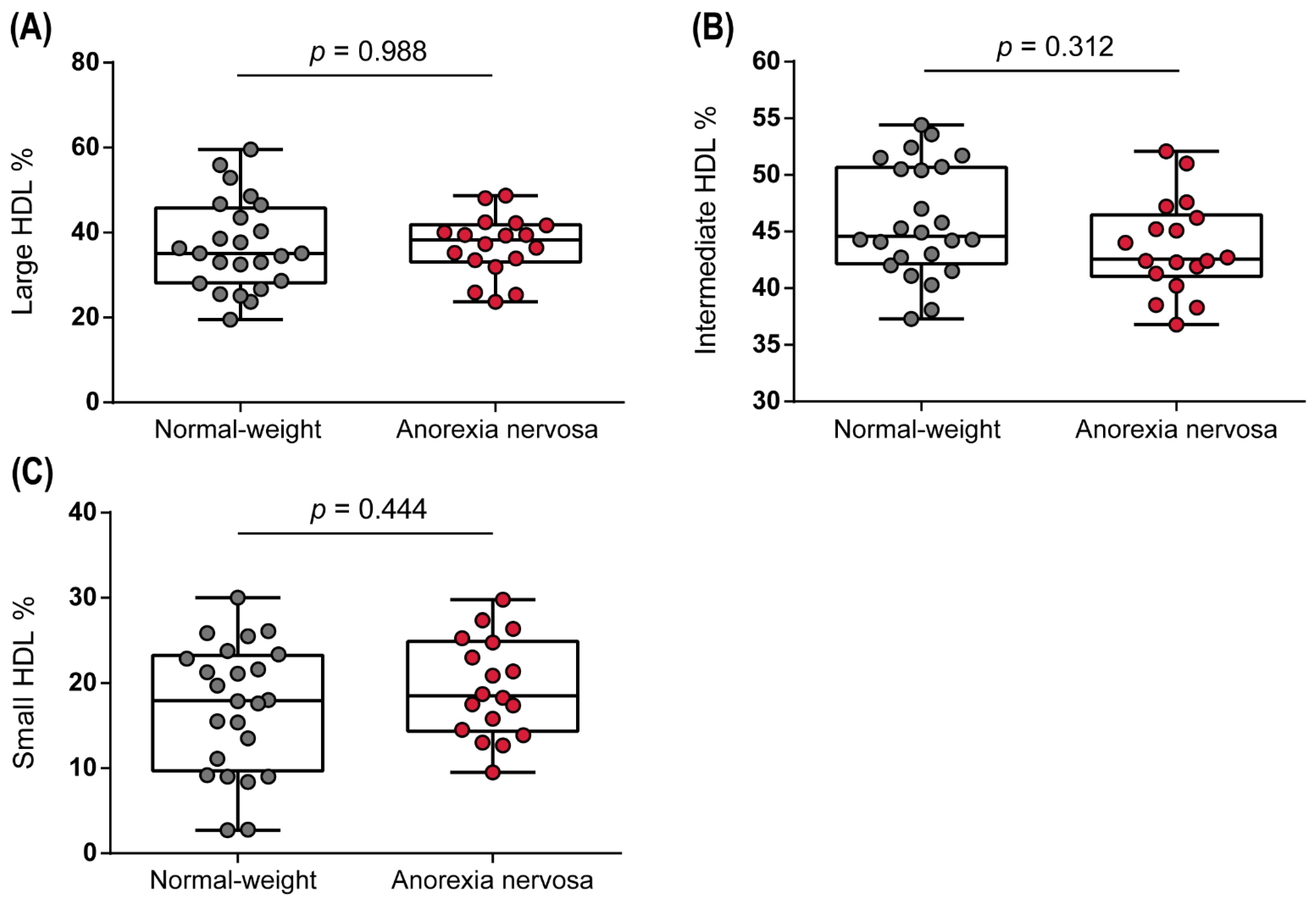
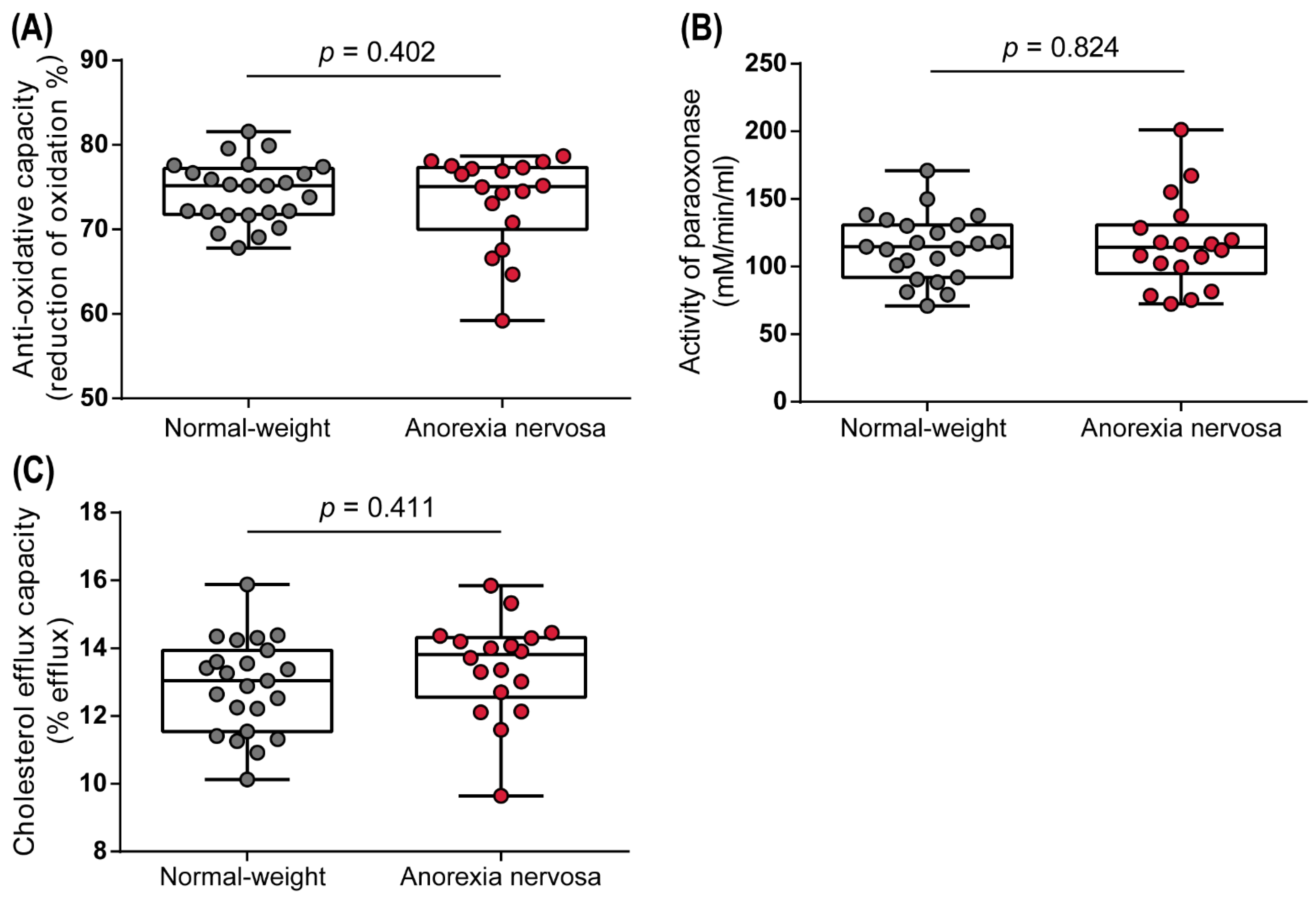
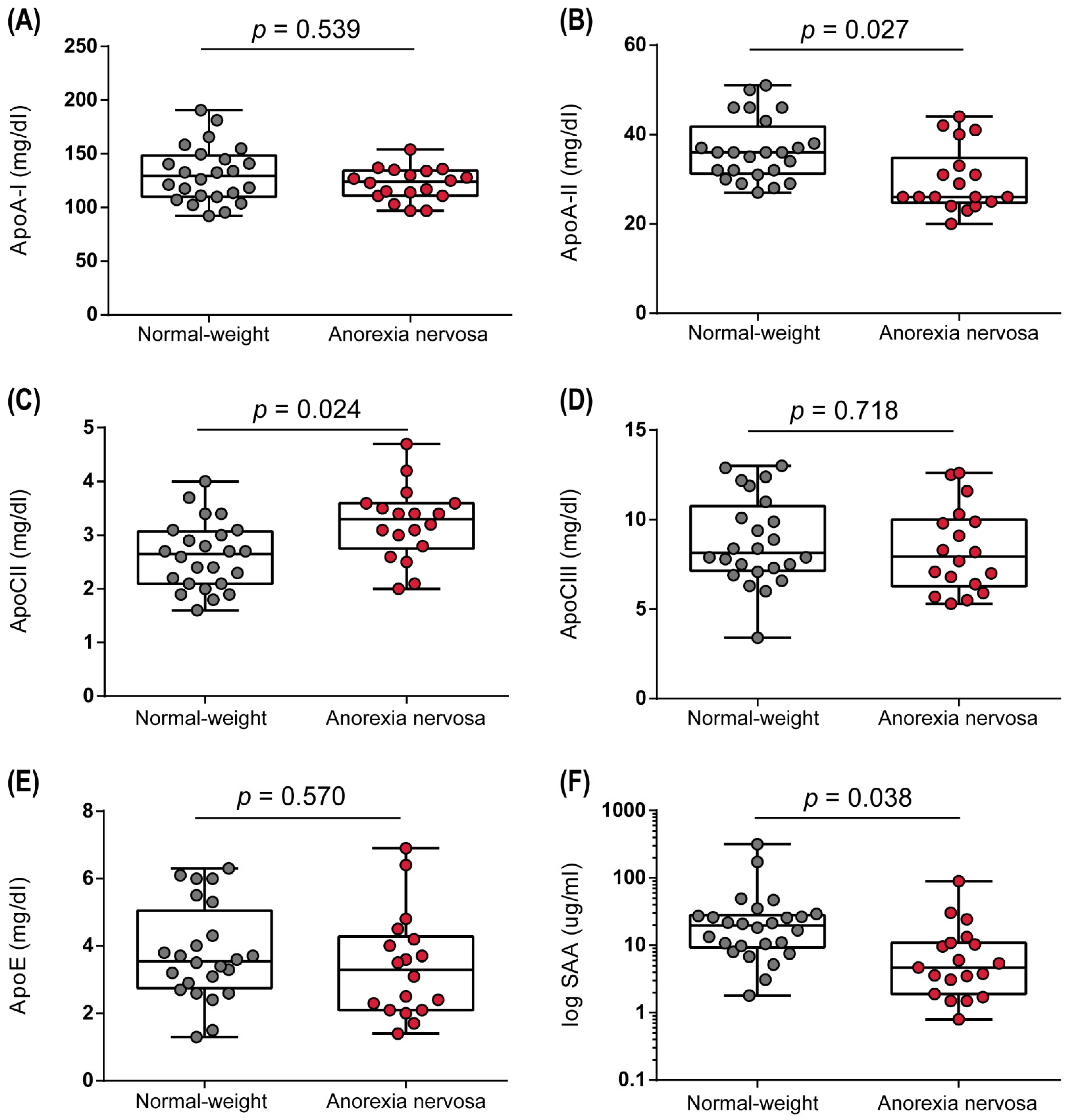
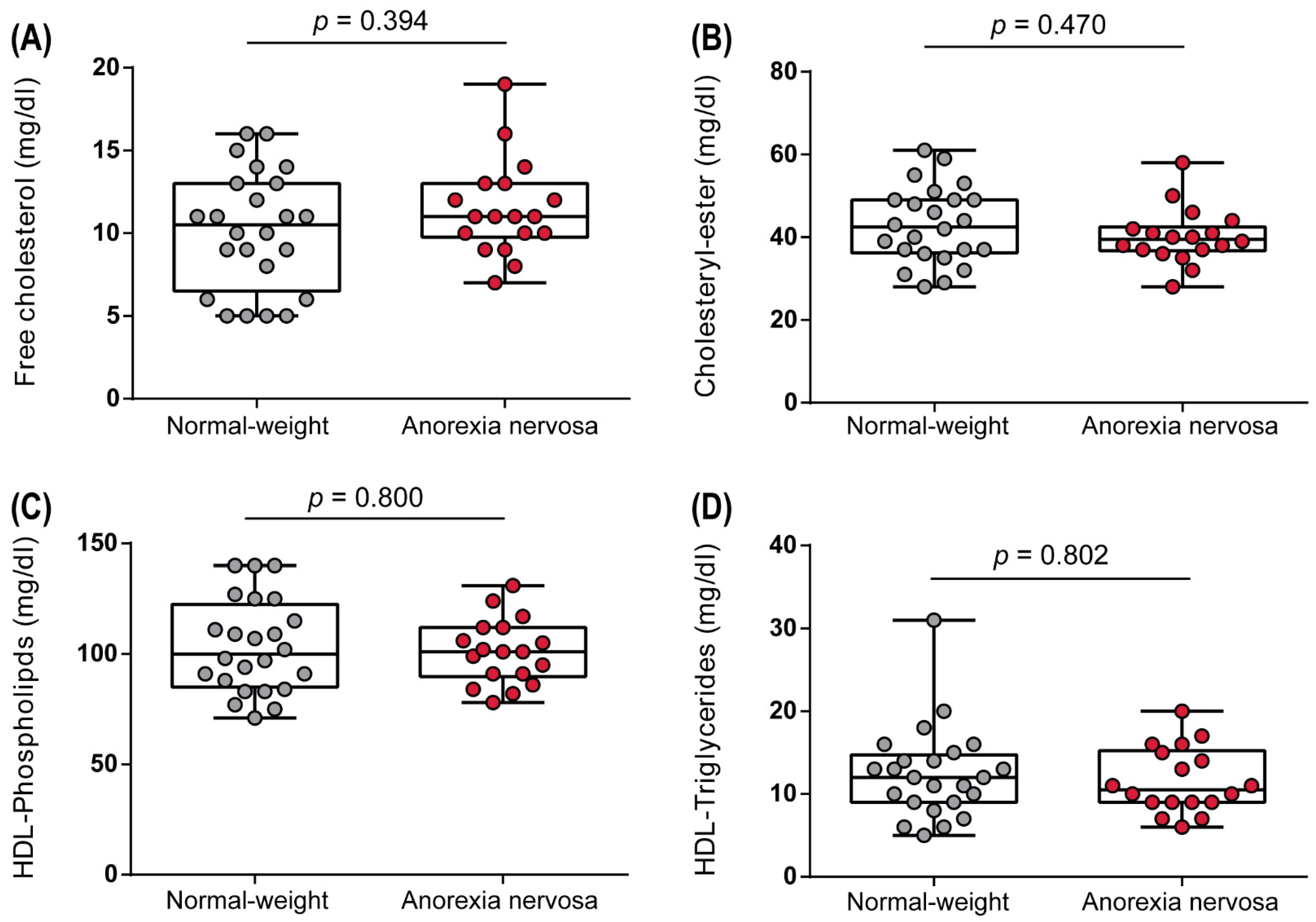
3.2. Anorexia Nervosa Was Associated with Changes in HDL Composition, but Not with Significant Alterations in HDL Subclass Distribution or HDL Function
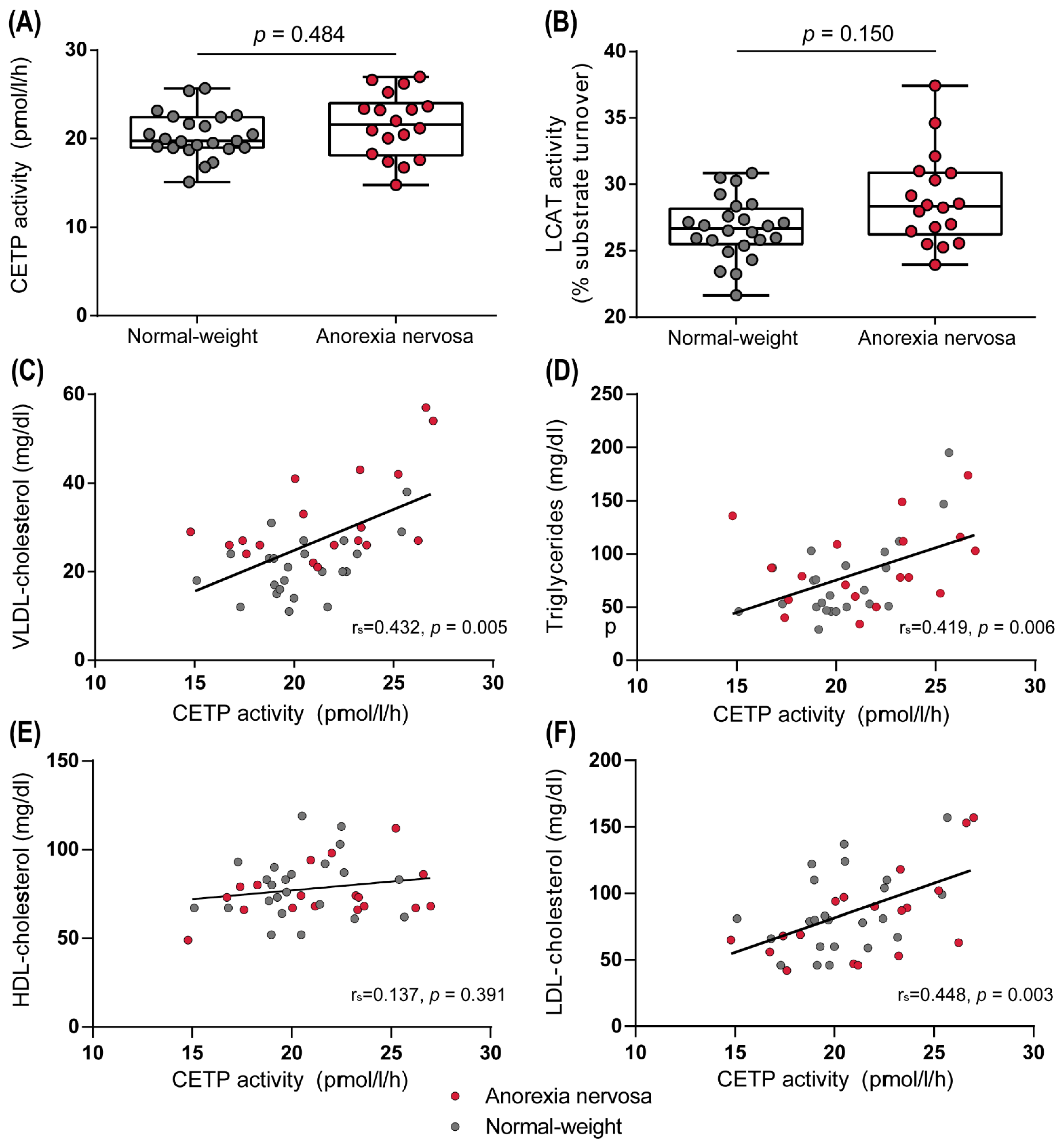
3.3. Effect of Anorexia Nervosa on Enzymes Involved in Lipoprotein Metabolism
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bulik, C.M.; Reba, L.; Siega-Riz, A.-M.; Reichborn-Kjennerud, T. Anorexia Nervosa: Definition, Epidemiology, and Cycle of Risk. Int. J. Eat. Disord. 2005, 37, S2–S9. [Google Scholar] [CrossRef] [PubMed]
- Chesney, E.; Goodwin, G.M.; Fazel, S. Risks of All-Cause and Suicide Mortality in Mental Disorders: A Meta-Review. World Psychiatry 2014, 13, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, A.A.; Hübel, C.; Hindborg, M.; Lindkvist, E.; Kastrup, A.M.; Yilmaz, Z.; Støving, R.K.; Bulik, C.M.; Sjögren, J.M. Increased Lipid and Lipoprotein Concentrations in Anorexia Nervosa: A Systematic Review and Meta-Analysis. Int. J. Eat. Disord. 2019, 52, 611–629. [Google Scholar] [CrossRef] [PubMed]
- Tomita, K.; Haga, H.; Ishii, G.; Katsumi, T.; Sato, C.; Aso, R.; Okumoto, K.; Nishise, Y.; Watanabe, H.; Saito, T.; et al. Clinical Manifestations of Liver Injury in Patients with Anorexia Nervosa. Hepatol. Res. 2014, 44, E26–E31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, E.; Sabel, A.L.; Brinton, J.T.; Catanach, B.; Gaudiani, J.L.; Mehler, P.S. Liver Dysfunction in Patients with Severe Anorexia Nervosa. Int. J. Eat. Disord. 2016, 49, 151–158. [Google Scholar] [CrossRef]
- Weinbrenner, T.; Züger, M.; Jacoby, G.E.; Herpertz, S.; Liedtke, R.; Sudhop, T.; Gouni-Berthold, I.; Axelson, M.; Berthold, H.K. Lipoprotein Metabolism in Patients with Anorexia Nervosa: A Case-Control Study Investigating the Mechanisms Leading to Hypercholesterolaemia. Br. J. Nutr. 2004, 91, 959–969. [Google Scholar] [CrossRef] [Green Version]
- Sachs, K.V.; Harnke, B.; Mehler, P.S.; Krantz, M.J. Cardiovascular Complications of Anorexia Nervosa: A Systematic Review. Int. J. Eat. Disord. 2016, 49, 238–248. [Google Scholar] [CrossRef]
- Nelson, R.H. Hyperlipidemia as a Risk Factor for Cardiovascular Disease. Prim. Care 2013, 40, 195–211. [Google Scholar] [CrossRef] [Green Version]
- Mortensen, M.B.; Nordestgaard, B.G. Elevated LDL Cholesterol and Increased Risk of Myocardial Infarction and Atherosclerotic Cardiovascular Disease in Individuals Aged 70–100 Years: A Contemporary Primary Prevention Cohort. Lancet 2020, 396, 1644–1652. [Google Scholar] [CrossRef]
- Werner, R.M.; Pearson, T.A. LDL-Cholesterol: A Risk Factor for Coronary Artery Disease—From Epidemiology to Clinical Trials. Can. J. Cardiol. 1998, 14 (Suppl. B), 3B–10B. [Google Scholar]
- Austin, M.A.; Breslow, J.L.; Hennekens, C.H.; Buring, J.E.; Willett, W.C.; Krauss, R.M. Low-Density Lipoprotein Subclass Patterns and Risk of Myocardial Infarction. JAMA 1988, 260, 1917–1921. [Google Scholar] [CrossRef] [PubMed]
- Campos, H.; Genest, J.J.; Blijlevens, E.; McNamara, J.R.; Jenner, J.L.; Ordovas, J.M.; Wilson, P.W.; Schaefer, E.J. Low Density Lipoprotein Particle Size and Coronary Artery Disease. Arterioscler. Thromb. 1992, 12, 187–195. [Google Scholar] [CrossRef]
- Ensign, W.; Hill, N.; Heward, C.B. Disparate LDL Phenotypic Classification among 4 Different Methods Assessing LDL Particle Characteristics. Clin. Chem. 2006, 52, 1722–1727. [Google Scholar] [CrossRef] [PubMed]
- Carmena, R.; Duriez, P.; Fruchart, J.-C. Atherogenic Lipoprotein Particles in Atherosclerosis. Circulation 2004, 109, III-2–III-7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamarche, B.; St-Pierre, A.C.; Ruel, I.L.; Cantin, B.; Dagenais, G.R.; Després, J.P. A Prospective, Population-Based Study of Low Density Lipoprotein Particle Size as a Risk Factor for Ischemic Heart Disease in Men. Can. J. Cardiol. 2001, 17, 859–865. [Google Scholar] [PubMed]
- Lamarche, B.; Tchernof, A.; Moorjani, S.; Cantin, B.; Dagenais, G.R.; Lupien, P.J.; Despre’s, J.-P. Small, Dense Low-Density Lipoprotein Particles as a Predictor of the Risk of Ischemic Heart Disease in Men. Circulation 1997, 95, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Ivanova, E.A.; Myasoedova, V.A.; Melnichenko, A.A.; Grechko, A.V.; Orekhov, A.N. Small Dense Low-Density Lipoprotein as Biomarker for Atherosclerotic Diseases. Oxidative Med. Cell. Longev. 2017, 2017, 1273042. [Google Scholar] [CrossRef]
- Stadler, J.T.; Lackner, S.; Mörkl, S.; Trakaki, A.; Scharnagl, H.; Borenich, A.; Wonisch, W.; Mangge, H.; Zelzer, S.; Meier-Allard, N.; et al. Obesity Affects HDL Metabolism, Composition and Subclass Distribution. Biomedicines 2021, 9, 242. [Google Scholar] [CrossRef]
- Ren, J.; Grundy, S.M.; Liu, J.; Wang, W.; Wang, M.; Sun, J.; Liu, J.; Li, Y.; Wu, Z.; Zhao, D. Long-Term Coronary Heart Disease Risk Associated with Very-Low-Density Lipoprotein Cholesterol in Chinese: The Results of a 15-Year Chinese Multi-Provincial Cohort Study (CMCS). Atherosclerosis 2010, 211, 327–332. [Google Scholar] [CrossRef]
- Brites, F.; Martin, M.; Guillas, I.; Kontush, A. Antioxidative Activity of High-Density Lipoprotein (HDL): Mechanistic Insights into Potential Clinical Benefit. BBA Clin. 2017, 8, 66–77. [Google Scholar] [CrossRef]
- Barter, P.J.; Nicholls, S.; Rye, K.A.; Anantharamaiah, G.M.; Navab, M.; Fogelman, A.M. Antiinflammatory Properties of HDL. Circ. Res. 2004, 95, 764–772. [Google Scholar] [CrossRef]
- Mineo, C.; Deguchi, H.; Griffin, J.H.; Shaul, P.W. Endothelial and Antithrombotic Actions of HDL. Circ. Res. 2006, 98, 1352–1364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohatgi, A.; Khera, A.; Berry, J.D.; Givens, E.G.; Ayers, C.R.; Wedin, K.E.; Neeland, I.J.; Yuhanna, I.S.; Rader, D.R.; de Lemos, J.A.; et al. HDL Cholesterol Efflux Capacity and Incident Cardiovascular Events. N. Engl. J. Med. 2014, 371, 2383–2393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems; World Health Organization: Geneva, Switzerland, 2015; ISBN 978-92-4-154916-5. [Google Scholar]
- Mörkl, S.; Lackner, S.; Müller, W.; Gorkiewicz, G.; Kashofer, K.; Oberascher, A.; Painold, A.; Holl, A.; Holzer, P.; Meinitzer, A.; et al. Gut Microbiota and Body Composition in Anorexia Nervosa Inpatients in Comparison to Athletes, Overweight, Obese, and Normal Weight Controls. Int. J. Eat. Disord. 2017, 50, 1421–1431. [Google Scholar] [CrossRef] [PubMed]
- Mörkl, S.; Lackner, S.; Meinitzer, A.; Mangge, H.; Lehofer, M.; Halwachs, B.; Gorkiewicz, G.; Kashofer, K.; Painold, A.; Holl, A.K.; et al. Gut Microbiota, Dietary Intakes and Intestinal Permeability Reflected by Serum Zonulin in Women. Eur. J. Nutr. 2018, 57, 2985–2997. [Google Scholar] [CrossRef] [Green Version]
- Lackner, S.; Mörkl, S.; Müller, W.; Fürhapter-Rieger, A.; Oberascher, A.; Lehofer, M.; Bieberger, C.; Wonisch, W.; Amouzadeh-Ghadikolai, O.; Moser, M.; et al. Novel Approaches for the Assessment of Relative Body Weight and Body Fat in Diagnosis and Treatment of Anorexia Nervosa: A Cross-Sectional Study. Clin. Nutr. 2019, 38, 2913–2921. [Google Scholar] [CrossRef] [Green Version]
- Lackner, S.; Meier-Allard, N.; Mörkl, S.; Müller, W.; Fürhapter-Rieger, A.; Mangge, H.; Zelzer, S.; Holasek, S. Hypercarotenemia in Anorexia Nervosa Patients May Influence Weight Balance: Results of a Clinical Cross-Sectional Cohort Study. Front. Psychiatry 2021, 12, 758300. [Google Scholar] [CrossRef]
- World Health Organization Body Mass Index—BMI. 2018. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 28 February 2022).
- Müller, W.; Lohman, T.G.; Stewart, A.D.; Maughan, R.J.; Meyer, N.L.; Sardinha, L.B.; Kirihennedige, N.; Reguant-Closa, A.; Risoul-Salas, V.; Sundgot-Borgen, J.; et al. Subcutaneous Fat Patterning in Athletes: Selection of Appropriate Sites and Standardisation of a Novel Ultrasound Measurement Technique: Ad Hoc Working Group on Body Composition, Health and Performance, under the Auspices of the IOC Medical Commission. Br. J. Sports Med. 2016, 50, 45–54. [Google Scholar] [CrossRef] [Green Version]
- Störchle, P.; Müller, W.; Sengeis, M.; Ahammer, H.; Fürhapter-Rieger, A.; Bachl, N.; Lackner, S.; Mörkl, S.; Holasek, S. Standardized Ultrasound Measurement of Subcutaneous Fat Patterning: High Reliability and Accuracy in Groups Ranging from Lean to Obese. Ultrasound Med. Biol. 2017, 43, 427–438. [Google Scholar] [CrossRef] [Green Version]
- Varady, K.A.; Lamarche, B. Lipoprint Adequately Estimates LDL Size Distribution, but Not Absolute Size, Versus Polyacrylamide Gradient Gel Electrophoresis. Lipids 2011, 46, 1163–1167. [Google Scholar] [CrossRef]
- Holzer, M.; Schilcher, G.; Curcic, S.; Trieb, M.; Ljubojevic, S.; Stojakovic, T.; Scharnagl, H.; Kopecky, C.M.; Rosenkranz, A.R.; Heinemann, A.; et al. Dialysis Modalities and HDL Composition and Function. J. Am. Soc. Nephrol. 2015, 26, 2267–2276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huber, R.; Nauck, M.; Lüdtke, R.; Scharnagl, H. Effects of One Week Juice Fasting on Lipid Metabolism: A Cohort Study in Healthy Subjects. Komplement. Kl. Nat. 2003, 10, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Trakaki, A.; Sturm, G.J.; Pregartner, G.; Scharnagl, H.; Eichmann, T.O.; Trieb, M.; Knuplez, E.; Holzer, M.; Stadler, J.T.; Heinemann, A.; et al. Allergic Rhinitis Is Associated with Complex Alterations in High-Density Lipoprotein Composition and Function. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 2019, 1864, 1280–1292. [Google Scholar] [CrossRef] [PubMed]
- Trieb, M.; Wolf, P.; Knuplez, E.; Weger, W.; Schuster, C.; Peinhaupt, M.; Holzer, M.; Trakaki, A.; Eichmann, T.; Lass, A.; et al. Abnormal Composition and Function of High-Density Lipoproteins in Atopic Dermatitis Patients. Allergy 2019, 74, 398–402. [Google Scholar] [CrossRef] [Green Version]
- Mahley, R.W.; Innerarity, T.L.; Rall, S.C.; Weisgraber, K.H. Plasma Lipoproteins: Apolipoprotein Structure and Function. J. Lipid Res. 1984, 25, 1277–1294. [Google Scholar] [CrossRef]
- Mead, J.R.; Irvine, S.A.; Ramji, D.P. Lipoprotein Lipase: Structure, Function, Regulation, and Role in Disease. J. Mol. Med. 2002, 80, 753–769. [Google Scholar] [CrossRef]
- Scanu, A. Serum High-Density Lipoprotein: Effect of Change in Structure on Activity of Chicken Adipose Tissue Lipase. Science 1966, 153, 640–641. [Google Scholar] [CrossRef]
- Larsson, M.; Allan, C.M.; Jung, R.S.; Heizer, P.J.; Beigneux, A.P.; Young, S.G.; Fong, L.G. Apolipoprotein C-III Inhibits Triglyceride Hydrolysis by GPIHBP1-Bound LPL. J. Lipid Res. 2017, 58, 1893–1902. [Google Scholar] [CrossRef] [Green Version]
- Camont, L.; Chapman, M.J.; Kontush, A. Biological Activities of HDL Subpopulations and Their Relevance to Cardiovascular Disease. Trends Mol. Med. 2011, 17, 594–603. [Google Scholar] [CrossRef]
- Swenne, I. Plasma Cholesterol Is Related to Menstrual Status in Adolescent Girls with Eating Disorders and Weight Loss. Acta Paediatr. 2016, 105, 317–323. [Google Scholar] [CrossRef]
- Balling, M.; Afzal, S.; Varbo, A.; Langsted, A.; Davey Smith, G.; Nordestgaard, B.G. VLDL Cholesterol Accounts for One-Half of the Risk of Myocardial Infarction Associated With ApoB-Containing Lipoproteins. J. Am. Coll. Cardiol. 2020, 76, 2725–2735. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, M.; Pernice, V.; Frasheri, A.; Di Lorenzo, G.; Rini, G.B.; Spinas, G.A.; Berneis, K. Small, Dense Low-Density Lipoproteins (LDL) Are Predictors of Cardio- and Cerebro-Vascular Events in Subjects with the Metabolic Syndrome. Clin. Endocrinol. 2009, 70, 870–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smythe, J.; Colebourn, C.; Prisco, L.; Petrinic, T.; Leeson, P. Cardiac Abnormalities Identified with Echocardiography in Anorexia Nervosa: Systematic Review and Meta-Analysis. Br. J. Psychiatry 2021, 219, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Giovinazzo, S.; Sukkar, S.G.; Rosa, G.M.; Zappi, A.; Bezante, G.P.; Balbi, M.; Brunelli, C. Anorexia Nervosa and Heart Disease: A Systematic Review. Eat. Weight. Disord. 2019, 24, 199–207. [Google Scholar] [CrossRef]
- Keel, P.K.; Forney, K.J. Psychosocial Risk Factors for Eating Disorders. Int. J. Eat. Disord. 2013, 46, 433–439. [Google Scholar] [CrossRef]
- Jacobi, C.; Hayward, C.; de Zwaan, M.; Kraemer, H.C.; Agras, W.S. Coming to Terms with Risk Factors for Eating Disorders: Application of Risk Terminology and Suggestions for a General Taxonomy. Psychol. Bull. 2004, 130, 19–65. [Google Scholar] [CrossRef]
- Striegel-Moore, R.H.; Bulik, C.M. Risk Factors for Eating Disorders. Am. Psychol. 2007, 62, 181–198. [Google Scholar] [CrossRef]
- Kontush, A.; Chapman, M.J. Antiatherogenic Small, Dense HDL--Guardian Angel of the Arterial Wall? Nat. Clin. Pract. Cardiovasc. Med. 2006, 3, 144–153. [Google Scholar] [CrossRef]
- Xepapadaki, E.; Kalogeropoulou, C.; Zvintzou, E.; Filou, S.; Kypreos, K.E. High Density Lipoprotein: The Role of Apolipoprotein A2. Hell. J. Atheroscler. 2018, 9, 128–137. [Google Scholar]
- Boisfer, E.; Lambert, G.; Atger, V.; Tran, N.Q.; Pastier, D.; Benetollo, C.; Trottier, J.F.; Beaucamps, I.; Antonucci, M.; Laplaud, M.; et al. Overexpression of Human Apolipoprotein A-II in Mice Induces Hypertriglyceridemia Due to Defective Very Low Density Lipoprotein Hydrolysis. J. Biol. Chem. 1999, 274, 11564–11572. [Google Scholar] [CrossRef] [Green Version]
- Marzal-Casacuberta, A.; Blanco-Vaca, F.; Ishida, B.Y.; Julve-Gil, J.; Shen, J.; Calvet-Márquez, S.; González-Sastre, F.; Chan, L. Functional Lecithin:Cholesterol Acyltransferase Deficiency and High Density Lipoprotein Deficiency in Transgenic Mice Overexpressing Human Apolipoprotein A-II. J. Biol. Chem. 1996, 271, 6720–6728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jong Miek, C.; Hofker Marten, H.; Havekes Louis, M. Role of ApoCs in Lipoprotein Metabolism. Arterioscler. Thromb. Vasc. Biol. 1999, 19, 472–484. [Google Scholar] [CrossRef] [Green Version]
- Ohwada, R.; Hotta, M.; Oikawa, S.; Takano, K. Etiology of Hypercholesterolemia in Patients with Anorexia Nervosa. Int. J. Eat. Disord. 2006, 39, 598–601. [Google Scholar] [CrossRef]
- Rigaud, D.; Tallonneau, I.; Vergès, B. Hypercholesterolaemia in Anorexia Nervosa: Frequency and Changes during Refeeding. Diabetes Metab. 2009, 35, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Glomset, J.A. The Plasma Lecithins:Cholesterol Acyltransferase Reaction. J. Lipid Res. 1968, 9, 155–167. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Characteristics | Anorexia Nervosa (n = 18) | Normal-Weight (n = 24) | p-Value |
|---|---|---|---|
| Age (years) | 22 (19–25) | 24 (22–26) | 0.082 |
| BMI (kg/m2) | 15.5 (14.3–16.2) | 21.8 (20.2–23.5) | <0.001 |
| DINCL (mm) | 30.2 (9.9–46.0) | 83.6 (66.1–99.1) | <0.001 |
| HDL-cholesterol (mg/dL) | 73.0 (67.0–81.5) | 79.5 (67.0–89.3) | 0.461 |
| LDL-cholesterol (mg/dL) | 78.0 (55.3–98.3) | 80.0 (60.8–108.5) | 0.797 |
| Triglycerides (mg/dL) | 78.5 (59.3–113.0) | 63.5 (50.0–98.8) | 0.199 |
| Total cholesterol (mg/dL) | 169.0 (145.3–202.0) | 167.0 (151.3–207.0) | 0.692 |
| CRP (mg/L) | 0.6 (0.6–1.6) | 1.4 (0.6–2.5) | 0.013 |
| Hba1c | 31.0 (29.5–34.3) | 31.0 (29.3–33.0) | 0.547 |
| Leptin (ng/mL) | 1.6 (1.0–3.8) | 10.6 (7.4–14.4) | <0.001 |
| sOB-R (ng/mL) | 30.8 (24.4–39.3) | 19.3 (16.4–21.8) | <0.001 |
| Adiponectin (μg/mL) | 16.5 (12.7–20.8) | 11.5 (9.3–16.7) | 0.019 |
| AP (U/L) | 52.5 (42.8–57.3) | 50.0 (44.0–55.8) | 0.865 |
| GGT (U/L) | 19.5 (11.5–24.3) | 12.5 (11.0–16.8) | 0.023 |
| CHE (U/L) | 6727 (5900–7201) | 7229 (6676–7901) | 0.038 |
| ALT (U/L) | 23.0 (15.0–34.0) | 14.0 (12.0–19.8) | 0.003 |
| AST (U/L) | 21.0 (20.0–23.3) | 20.0 (17.3–24.3) | 0.151 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stadler, J.T.; Lackner, S.; Mörkl, S.; Meier-Allard, N.; Scharnagl, H.; Rani, A.; Mangge, H.; Zelzer, S.; Holasek, S.J.; Marsche, G. Anorexia Nervosa Is Associated with a Shift to Pro-Atherogenic Low-Density Lipoprotein Subclasses. Biomedicines 2022, 10, 895. https://doi.org/10.3390/biomedicines10040895
Stadler JT, Lackner S, Mörkl S, Meier-Allard N, Scharnagl H, Rani A, Mangge H, Zelzer S, Holasek SJ, Marsche G. Anorexia Nervosa Is Associated with a Shift to Pro-Atherogenic Low-Density Lipoprotein Subclasses. Biomedicines. 2022; 10(4):895. https://doi.org/10.3390/biomedicines10040895
Chicago/Turabian StyleStadler, Julia T., Sonja Lackner, Sabrina Mörkl, Nathalie Meier-Allard, Hubert Scharnagl, Alankrita Rani, Harald Mangge, Sieglinde Zelzer, Sandra J. Holasek, and Gunther Marsche. 2022. "Anorexia Nervosa Is Associated with a Shift to Pro-Atherogenic Low-Density Lipoprotein Subclasses" Biomedicines 10, no. 4: 895. https://doi.org/10.3390/biomedicines10040895